

Charlotte is a junior doctor and an established member of the Soton Brain Hub team. She loves wo rking with the Apple Pencil to create digital learning resources and wow - is she good at it! She also loves using emojis😘😍😭👌.
rking with the Apple Pencil to create digital learning resources and wow - is she good at it! She also loves using emojis😘😍😭👌.
On this page we are sharing her clinically focused flashcards that help explain neuroanatomy and head & neck anatomy in an applied form to support medical students to integrate their knowledge. These images and their associated notes can also be found on our instagram page too.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
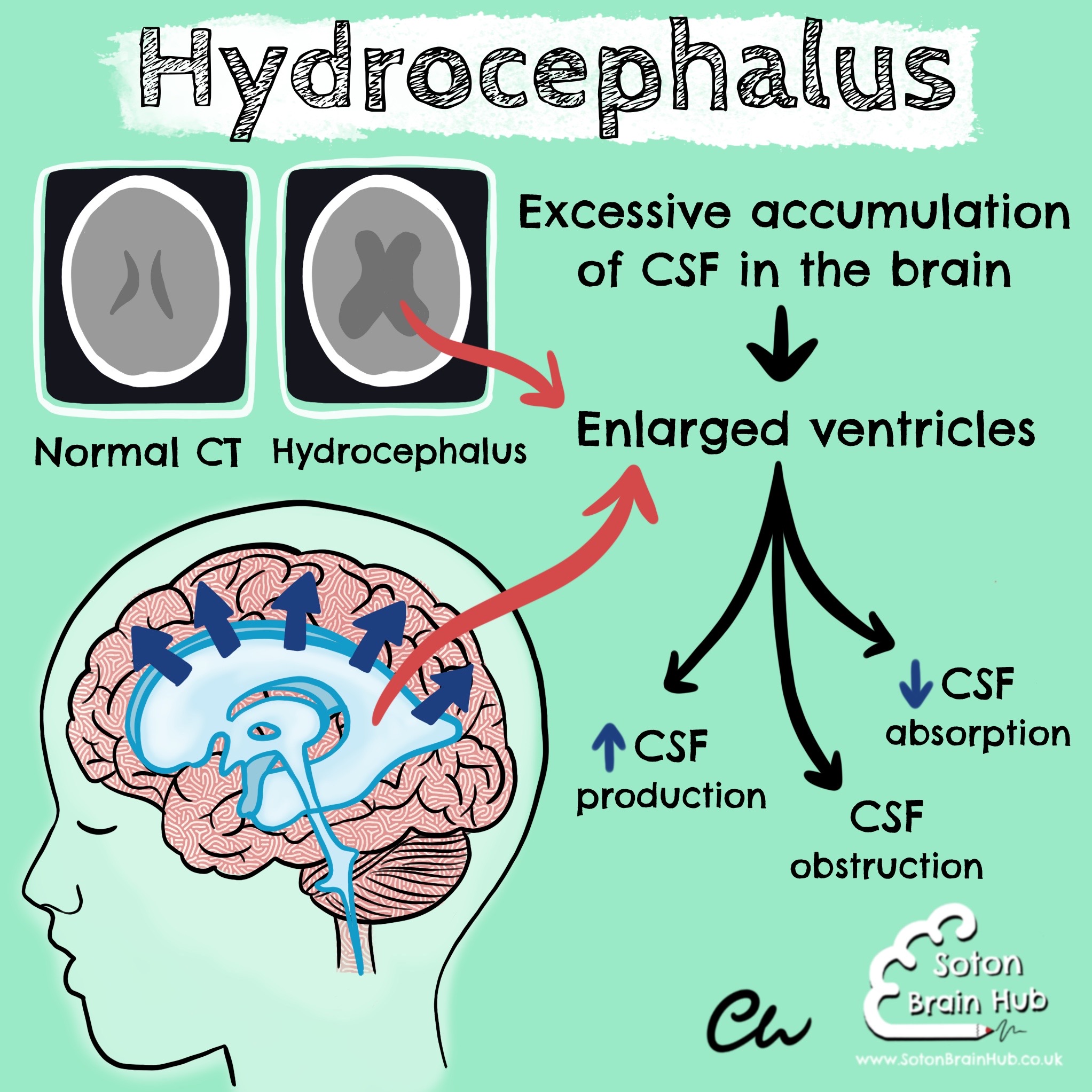
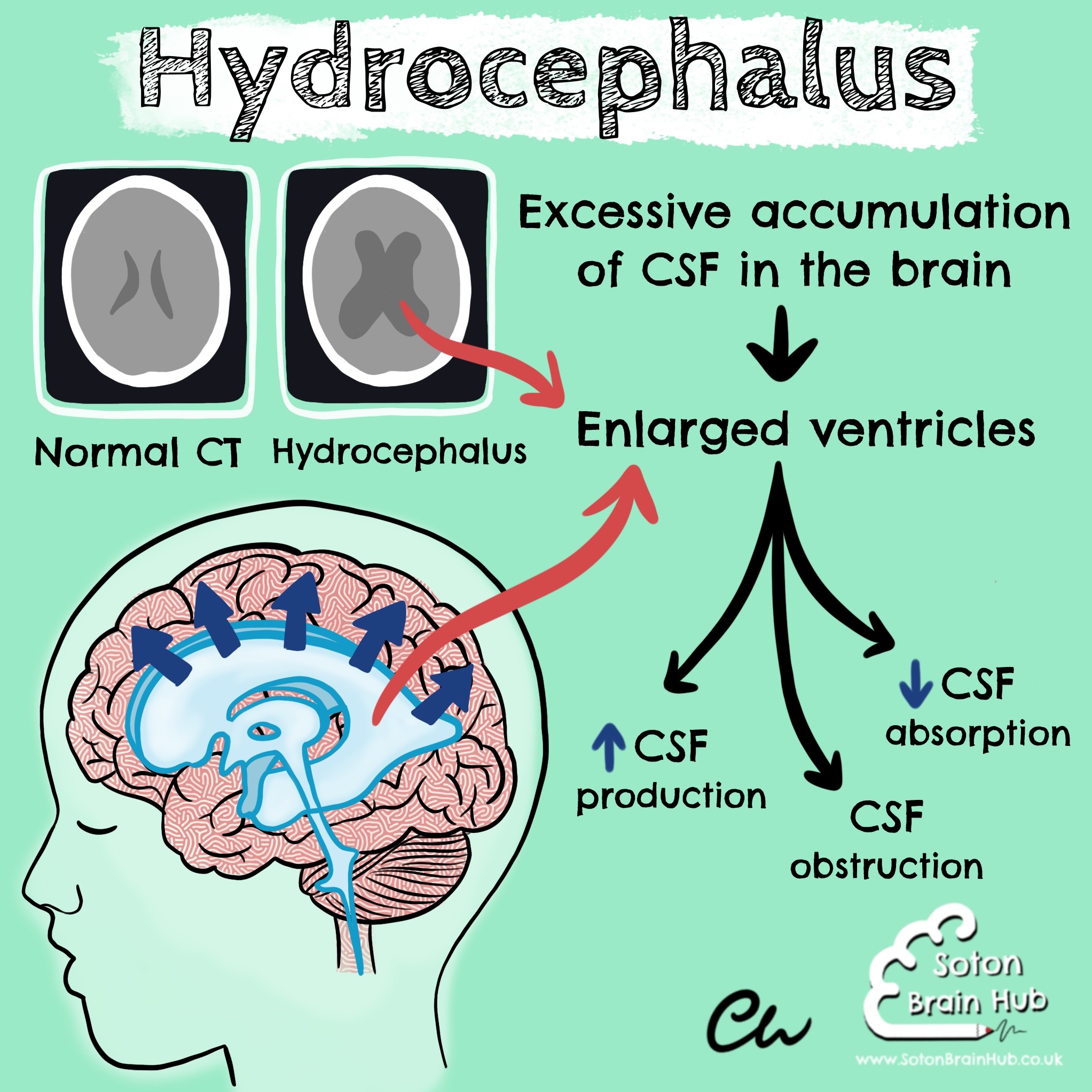
Hydrocephalus is an excessive accumulation of cerebrospinal fluid (CSF) in the brain  . It causes the ventricular system to enlarge, which typically causes increased intracranial pressure. If it is not treated, it can lead to permanent brain damage.
. It causes the ventricular system to enlarge, which typically causes increased intracranial pressure. If it is not treated, it can lead to permanent brain damage.
Symptoms of hydrocephalus can include headache  , vomiting
, vomiting  , blurred vision
, blurred vision  , poor
, poor
balance, urinary incontinence, seizures, and a rapid increase in head size in babies (since the fontanelles of the skull have not yet fused) 
Hydrocephalus can be congenital or acquired. Congenital hydrocephalus can be caused by spina bifida or maternal infections in pregnancy (mumps and rubella).
The pathophysiology of hydrocephalus can be categorised as: Increased CSF production (e.g. choroid plexus papilloma)
Increased CSF production (e.g. choroid plexus papilloma) Decreased CSF absorption (e.g. meningitis, subarachnoid haemorrhage, normal pressure hydrocephalus)
Decreased CSF absorption (e.g. meningitis, subarachnoid haemorrhage, normal pressure hydrocephalus) CSF obstruction (e.g. congenital aqueduct stenosis, tectal plate glioma, colloid cyst)
CSF obstruction (e.g. congenital aqueduct stenosis, tectal plate glioma, colloid cyst)
It is treated with shunt surgery or endoscopic third ventriculostomy (ETV)
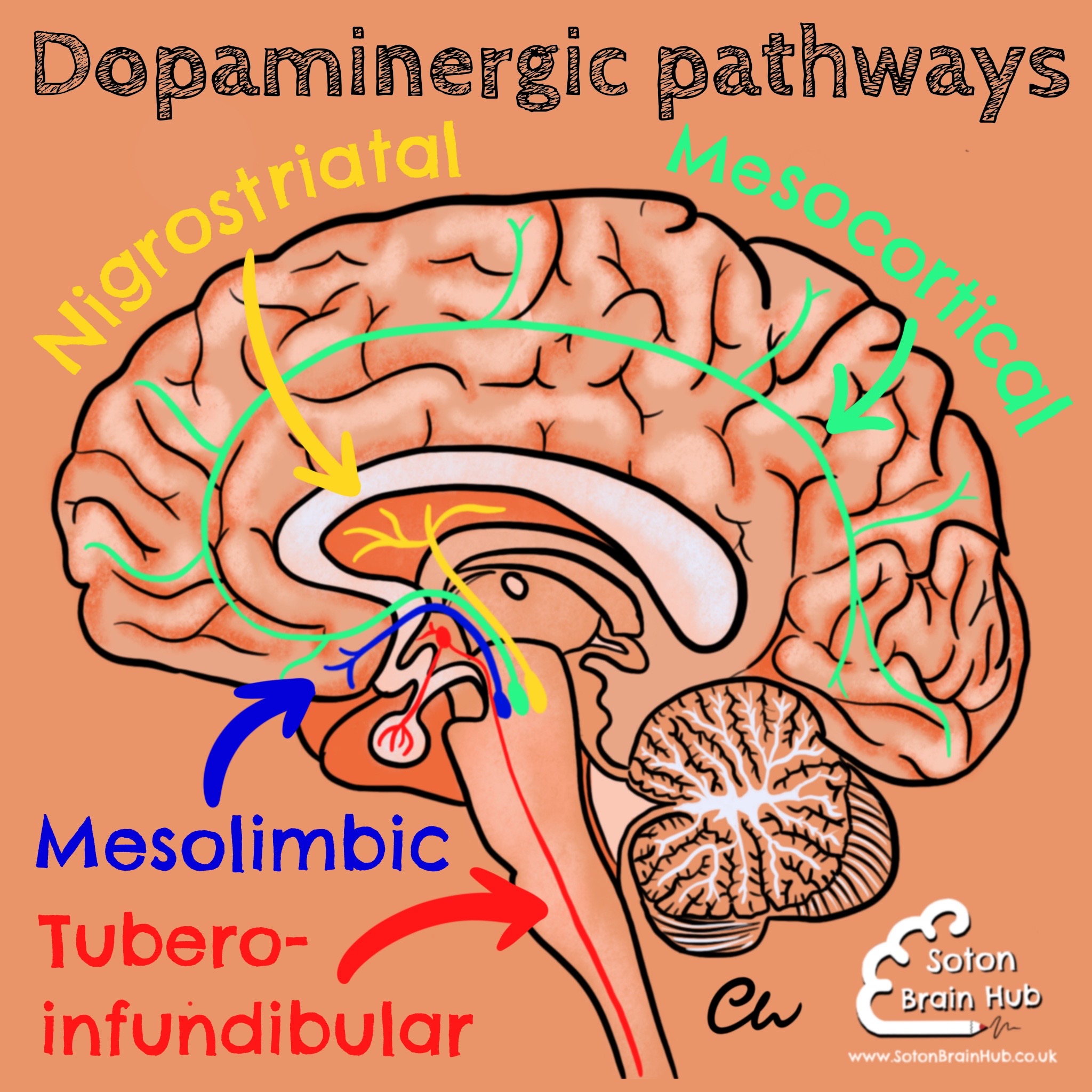
There are a number of dopaminergic pathways in the brain
The following  pathways are clinically relevant to to the action and side effects of antipsychotics, for the treatment of Schizophrenia. These are D2 antagonists that act by reducing dopamine levels. MESOLIMBIC PATHWAY
pathways are clinically relevant to to the action and side effects of antipsychotics, for the treatment of Schizophrenia. These are D2 antagonists that act by reducing dopamine levels. MESOLIMBIC PATHWAY 
Transmits dopamine from the midbrain (VTA) to the ventral striatum. It includes the nucleus accumbens (which is associated with motivations, emotions and rewards). This is thought to be responsible for the positive sympt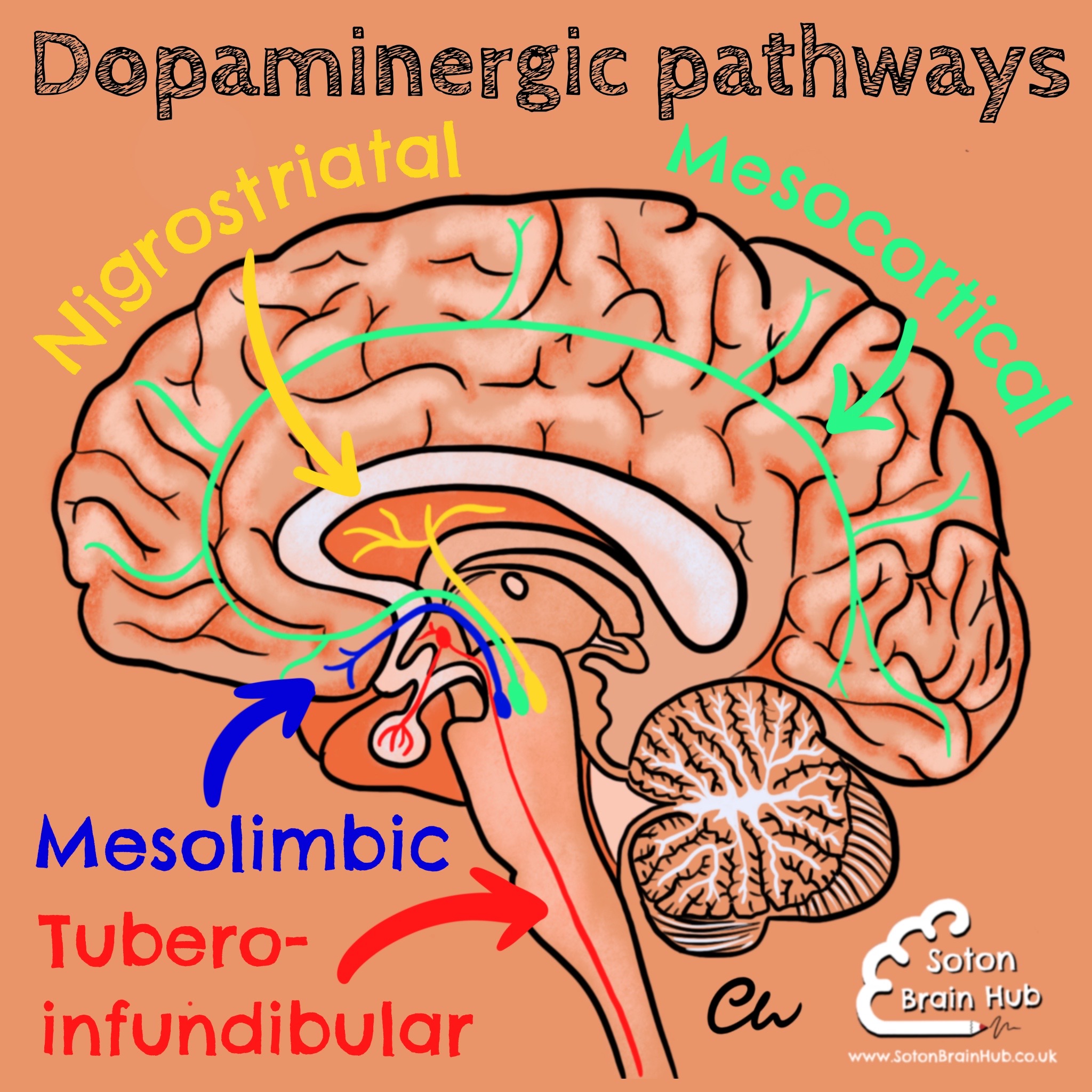 oms of Schizophrenia, which are reduced with antipsychotic use.
oms of Schizophrenia, which are reduced with antipsychotic use.
MESOCORTICAL PATHWAY 
Transmits dopamine from the midbrain (VTA) to the prefrontal cortex. Hypofunction of this pathway is thought to be responsible for the negative symptoms in Schizophrenia. NIGROSTRIATAL PATHWAY 
Transmits 80% of the brains dopamine from the pars compacta of the substantia nigra to the caudate nucleus and putamen. Antipsychotics that reduce dopamine can induce extrapyramidal side effects (similar to the pathophysiology of Parkinson’s disease). TUBEROINFUNDIBULAR PATHWAY 
Transmits dopamine from the hypothalamus to the pituitary gland. Dopamine in this pathway acts to inhibit prolactin. Blockade of D2 receptors by antipsychotics causes hyperprolactinaemia, and can result in breast enlargement, galactorrhoea, reduced libido and erectile dysfunction.
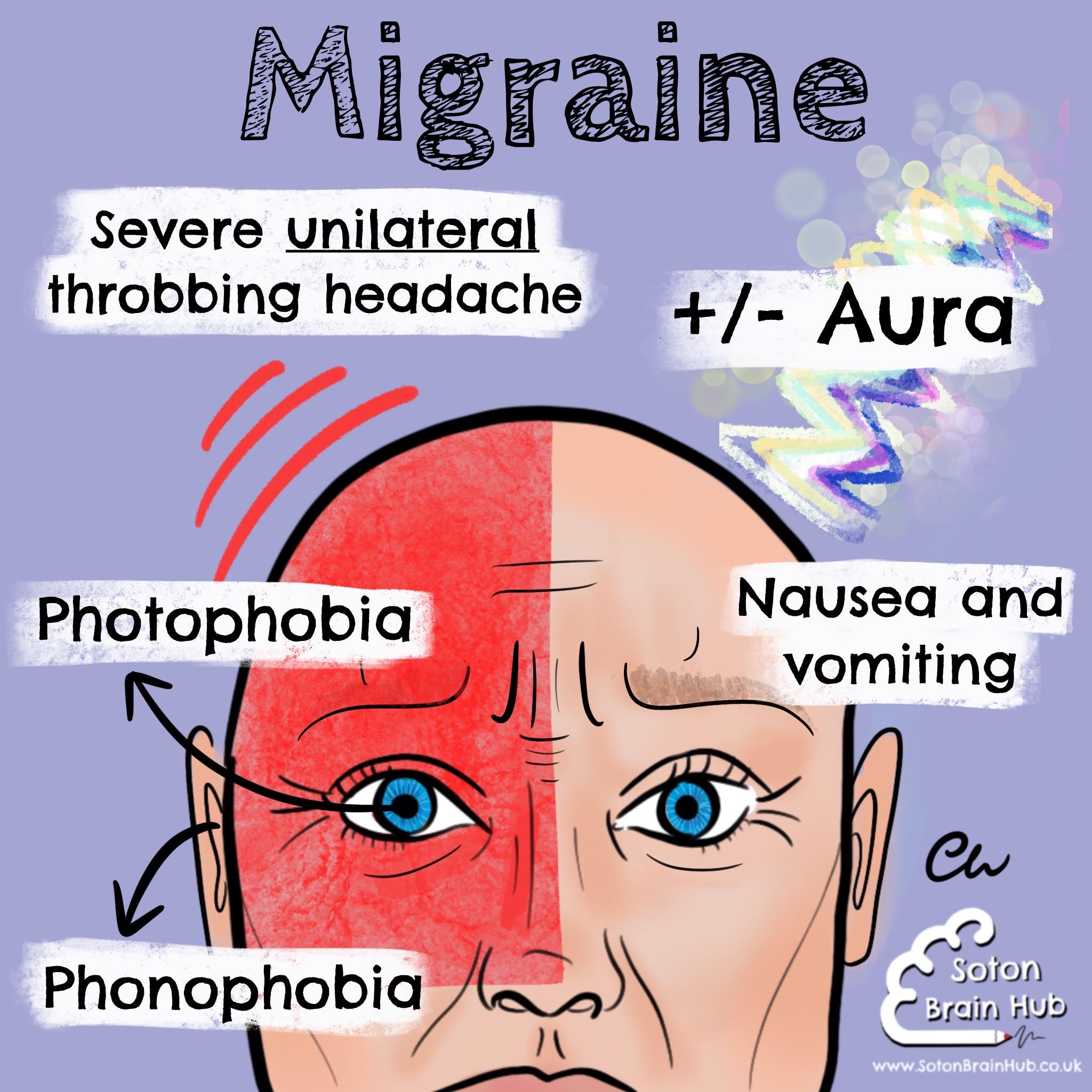
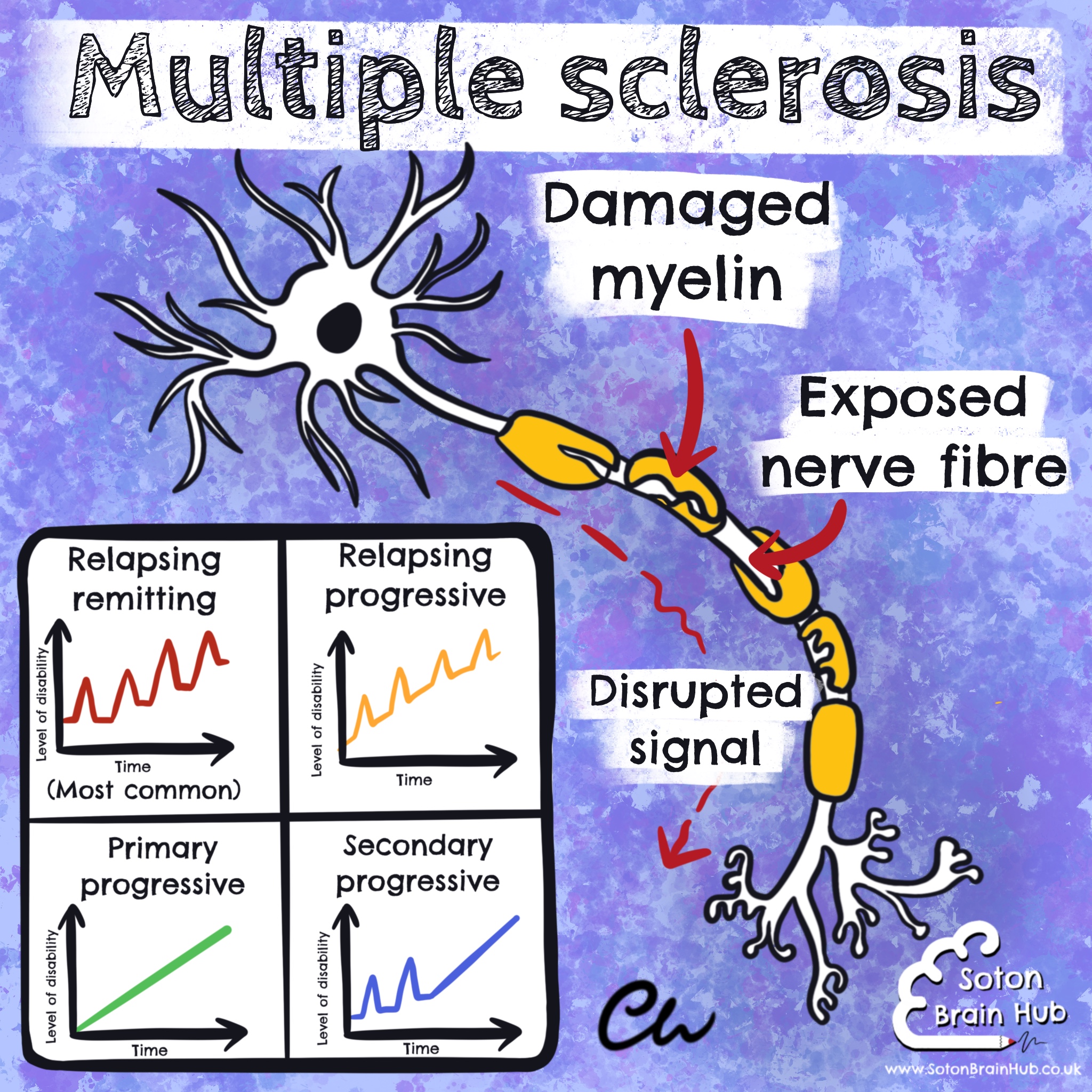
Migraine a common type of primary headache
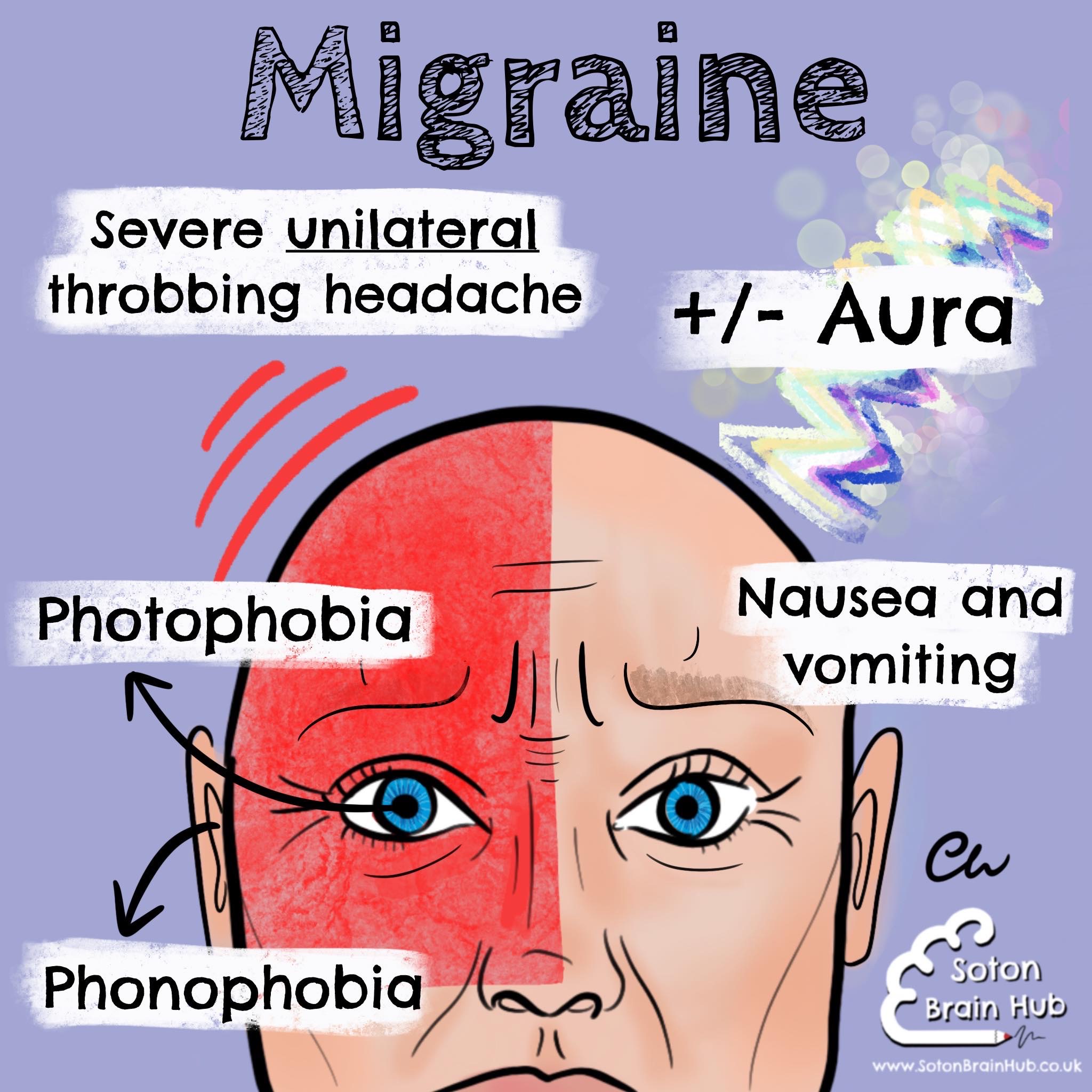 It typically causes a severe, unilateral, throbbing headache, and is associated with nausea, vomiting, photophobia and phonophobia. It can last up to 72 hours.
It typically causes a severe, unilateral, throbbing headache, and is associated with nausea, vomiting, photophobia and phonophobia. It can last up to 72 hours.
Migraines can occur with and without aura (neurological symptoms). Auras are most commonly visual disturbances and can include blind spots, flashes and scotoma 
 . However, auras may also consist of paraesthesia, weakness and vertigo.
. However, auras may also consist of paraesthesia, weakness and vertigo.
Common triggers for a migraine are tiredness, stress, alcohol, menstruation, the combined oral contraceptive pill,
hunger, dehydration, cheese  , chocolate
, chocolate , red wine
, red wine citrus
citrus  and bright lights. It 3 times more common in women.
and bright lights. It 3 times more common in women.
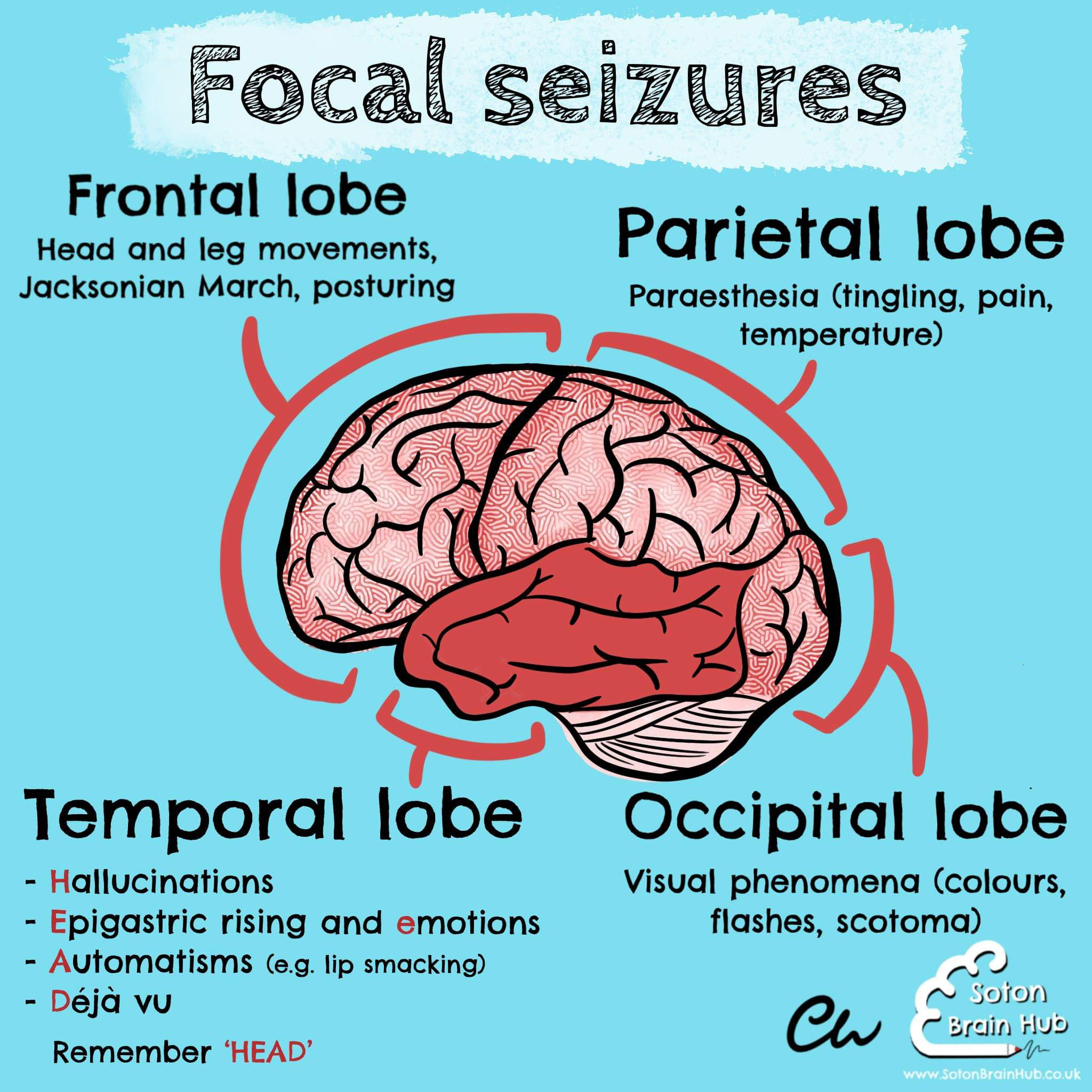
Focal seizures are seizures arising from a focal area within one hemisphere of the brain. They can progress to generalised seizures
Frontal lobe focal seizures may show signs including head or leg movement, abnormal posturing and Jacksonian march (a phenomenon in which the seizure starts at the distal part of a limb and progresses towards the ipsilateral face, like a “march”) 
Parietal lobe focal seizures often consist of sensory symptoms like tingling, pain and temperature changes 
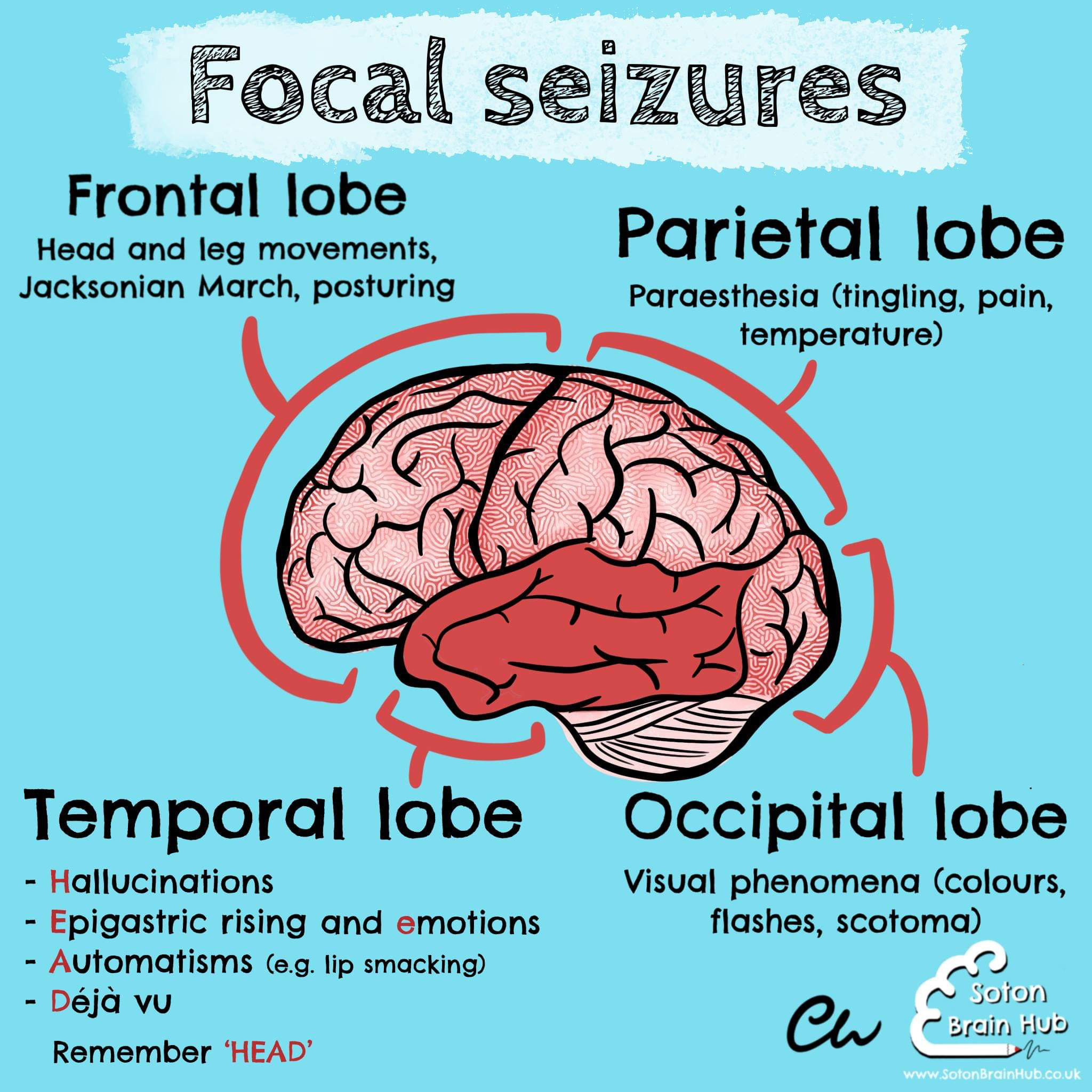
Occipital lobe focal seizures involve visual phenomena such as colours, flashes of light and scotoma 

Temporal lobe seizures are the most common of the focal seizures. Its signs can be remembered by “HEAD”’
- Hallucinations (which can be auditory, olfactory or gustatory)

- Emotions or an epigastric rising sensation 
- Automatisms (non-purposeful repetitive behaviours e.g. lip smacking) 
- Déjà vu
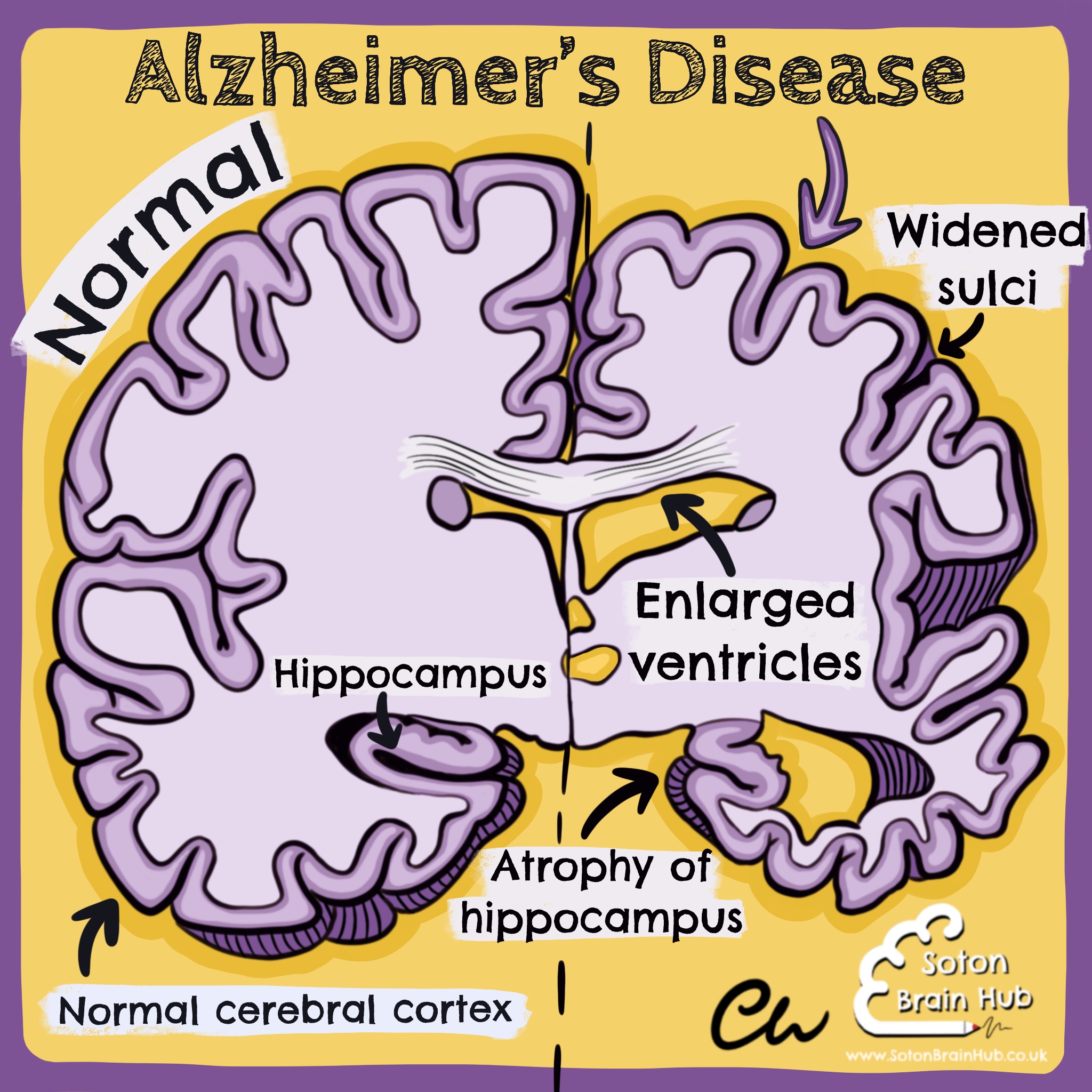
Alzheimer’s disease is the most common form of dementia. It has a slower and more insidious onset than many other types of dementia.
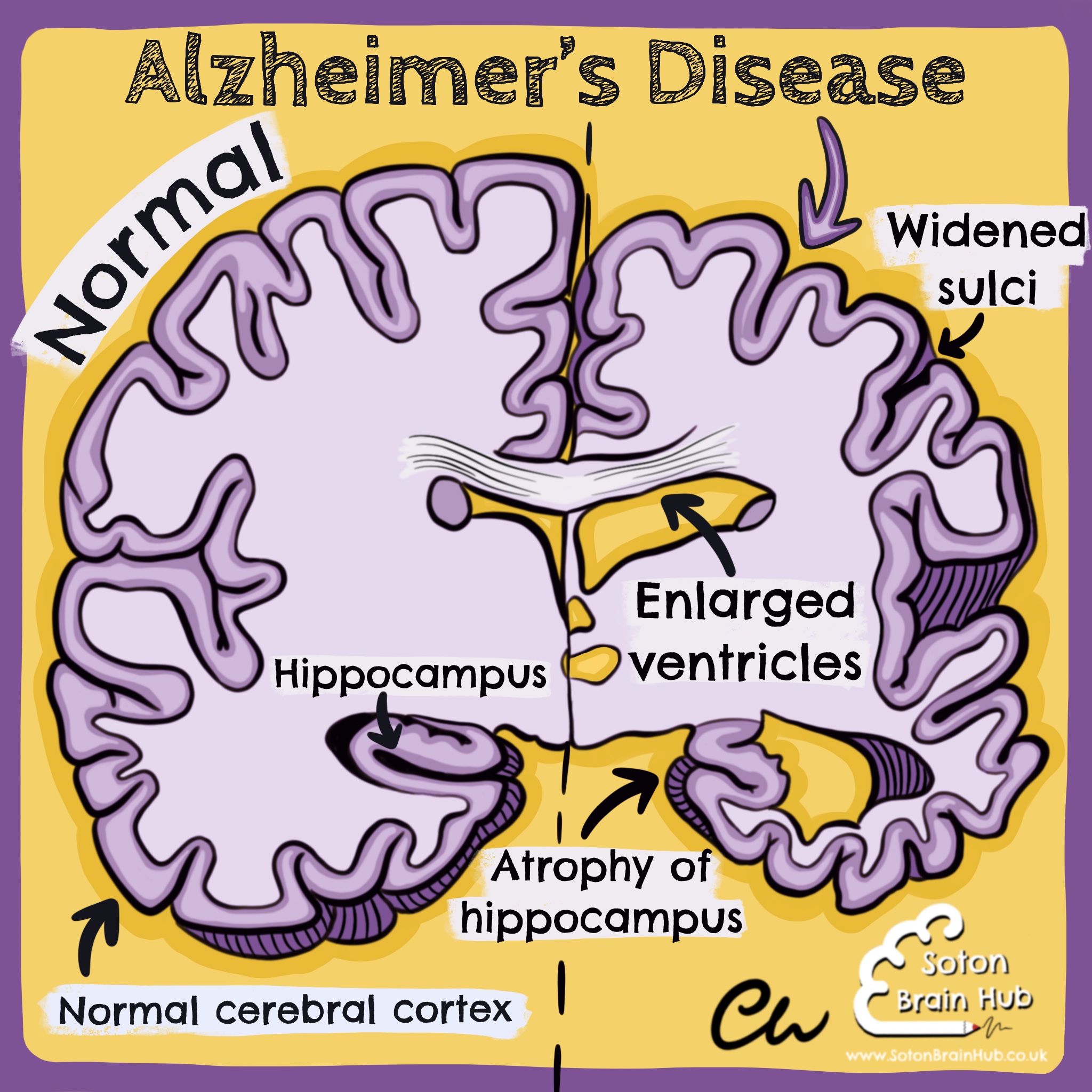
Macroscopically, the brain in Alzheimer’s disease exhibits generalised cerebral cortex atrophy (especially of the medial temporal lobe), widening of sulci, enlarged ventricles (a compensatory mechanism), and atrophy of the hippocampus .
The hippocampus is critical for the formation of new memories, so it is unsurprising that patients with Alzheimer’s often have deficits in short term memory.
Other early features include word finding difficulties  , decision making difficulties
, decision making difficulties , apathy and mood changes
, apathy and mood changes .
.
Later, patients may exhibit behavioural and psychological symptoms (like agitation and aggression), delusions, sleep disorders, physical frailty, incontinence, weight loss and communication difficulties.
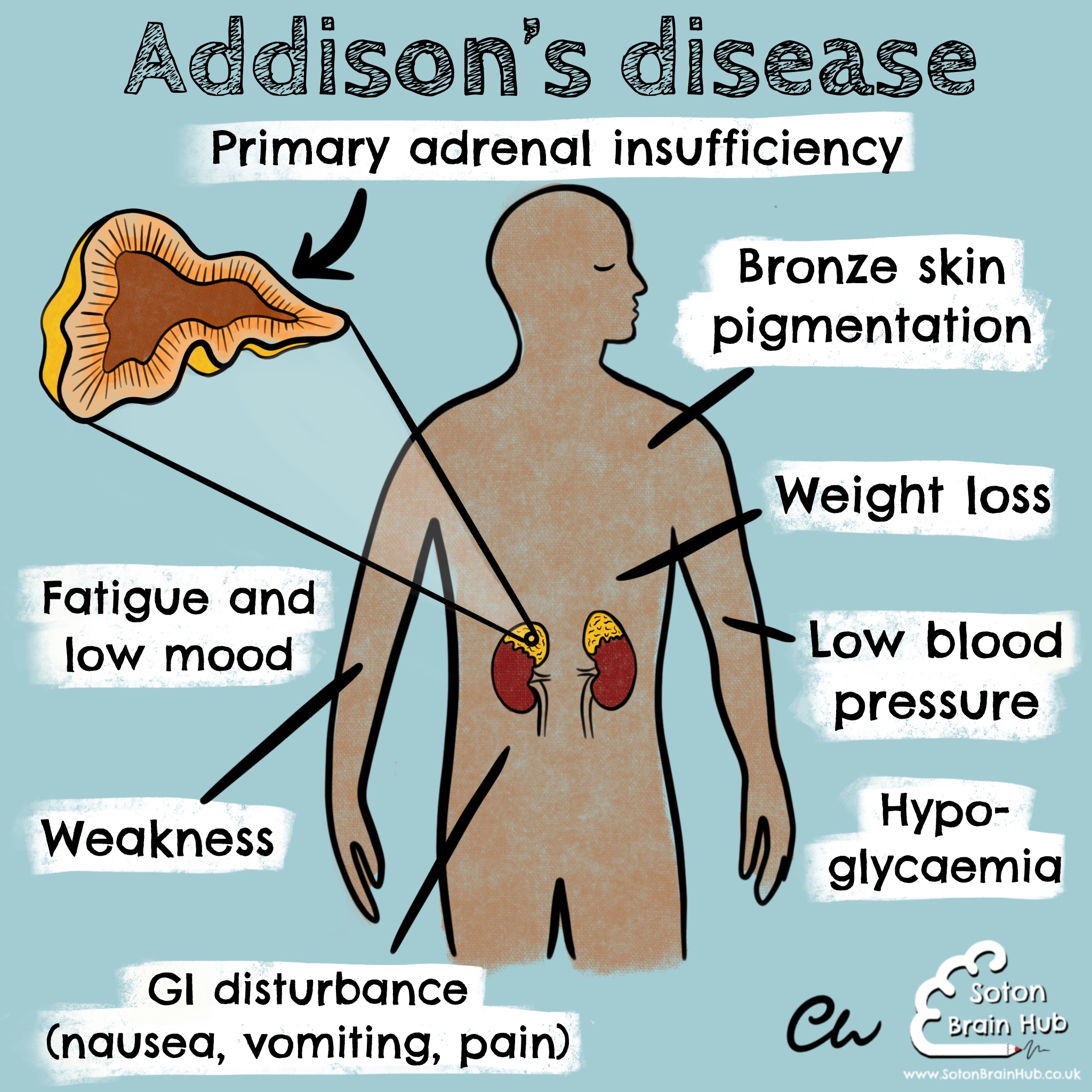
Addison’s disease is a rare disorder of the adrenal glands. It is also known as primary adrenal insufficiency. It can be life threatening.
Damage to the adrenal glands (usually autoimmune) results in insufficient production of steroid hormones (including cortisol and aldosterone).
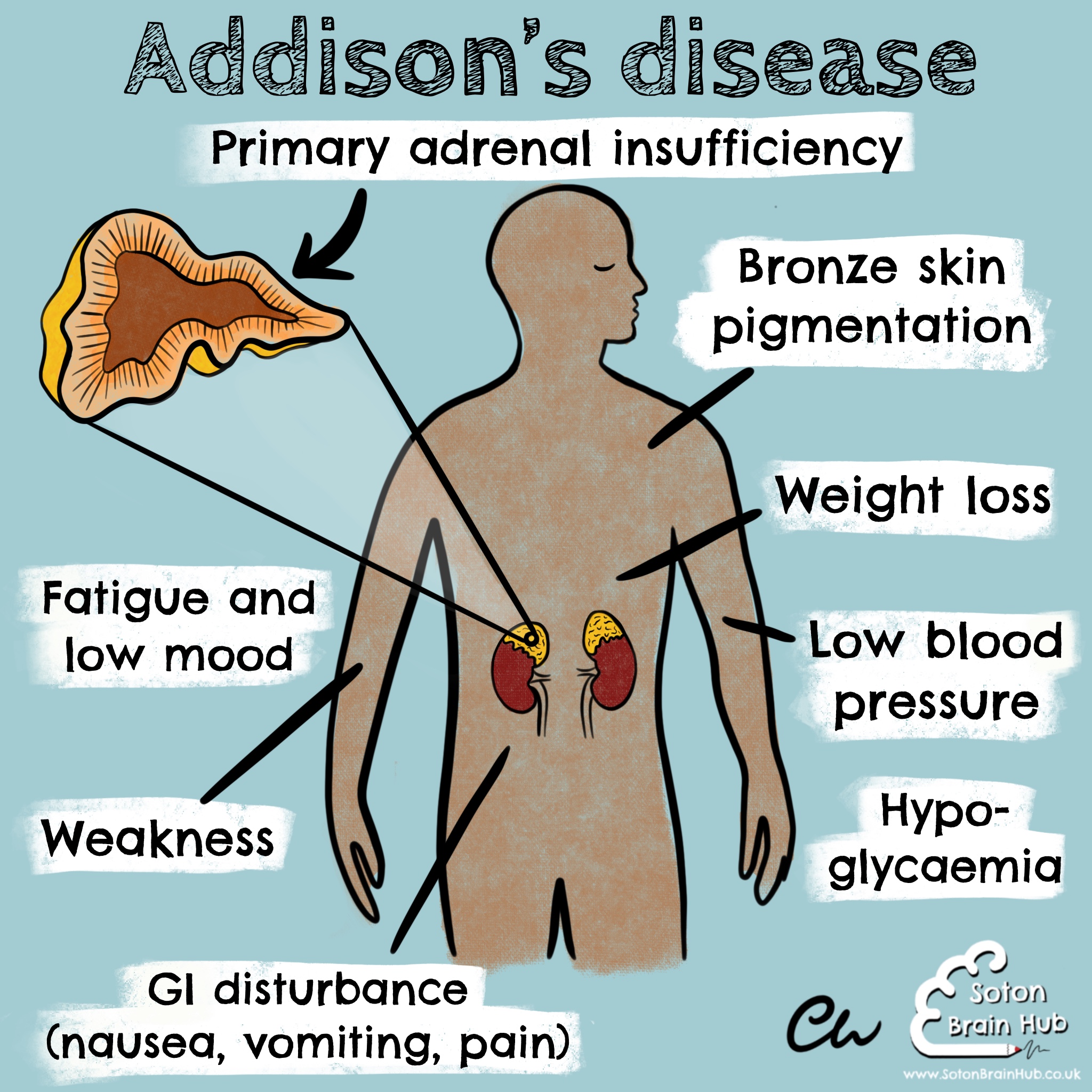 To try and maintain homeostasis, the hypothalamus stimulates the pituitary gland to release more ACTH to stimulate the adrenal glands to produce more steroid hormones.
To try and maintain homeostasis, the hypothalamus stimulates the pituitary gland to release more ACTH to stimulate the adrenal glands to produce more steroid hormones.
This also has the effect of increasing melanocyte-stimulating hormone, which results in the characteristic bronze skin pigmentation in Addison’s disease .
.
Other signs and symptoms include weight loss , low blood pressure, hypoglycaemia, GI disturbance (nausea
, low blood pressure, hypoglycaemia, GI disturbance (nausea , vomiting, abdominal pain, constipation), muscle weakness, increased thirst, fatigue and low mood
, vomiting, abdominal pain, constipation), muscle weakness, increased thirst, fatigue and low mood . Treatment involves lifelong replacement of the steroid hormones
. Treatment involves lifelong replacement of the steroid hormones
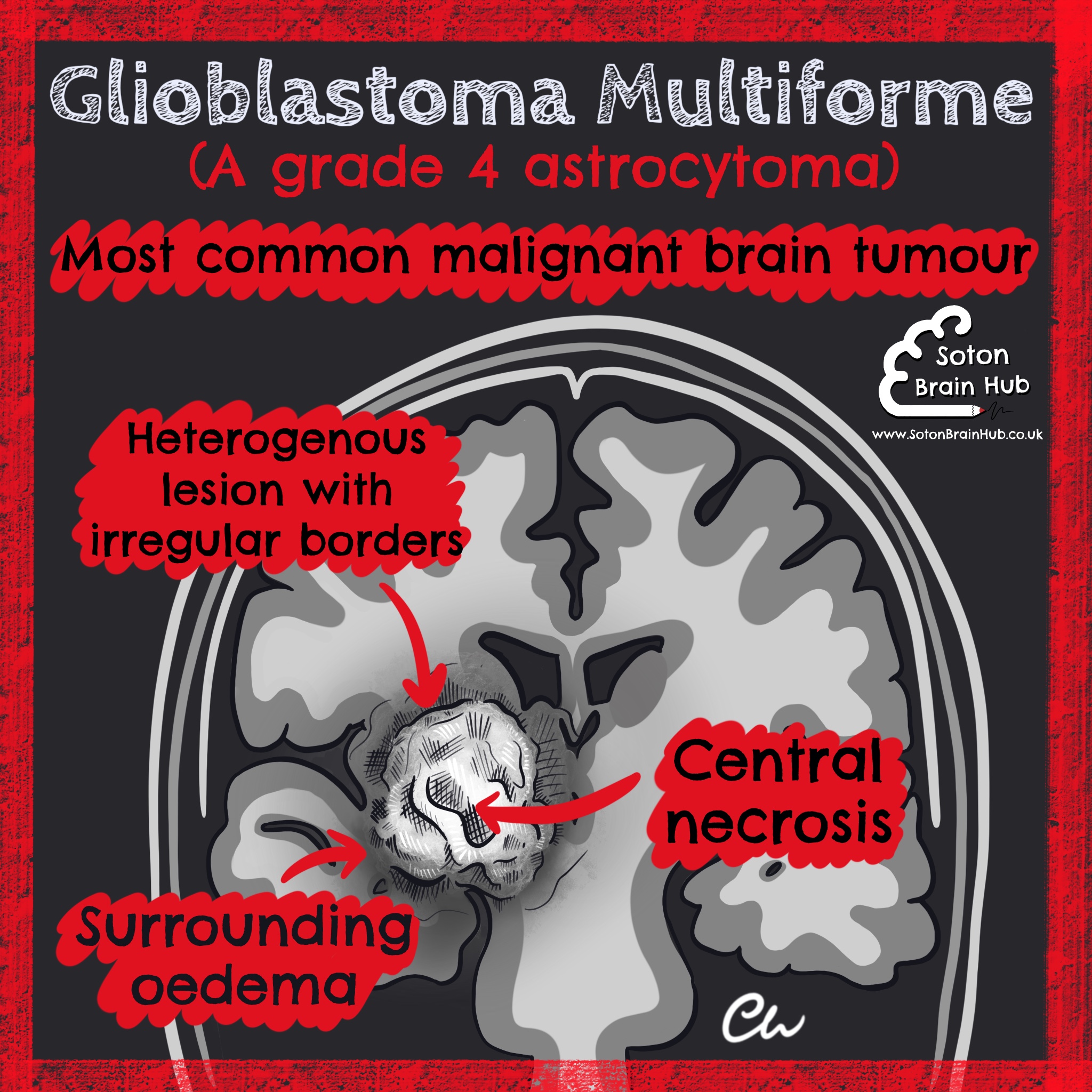
Glioblastoma Multiforme is the most common type of primarybrain tumour, with around 4,500 new cases in the UK per year. It is the most malignant type of astrocytoma (grade 4), which are brain tumours that develop from astrocytes.
Radiologically it appears as a heterogenous ring enhancing lesion within the brain with irregular margins, surrounded by an area of oedema. It typically has a central area of necrosis. 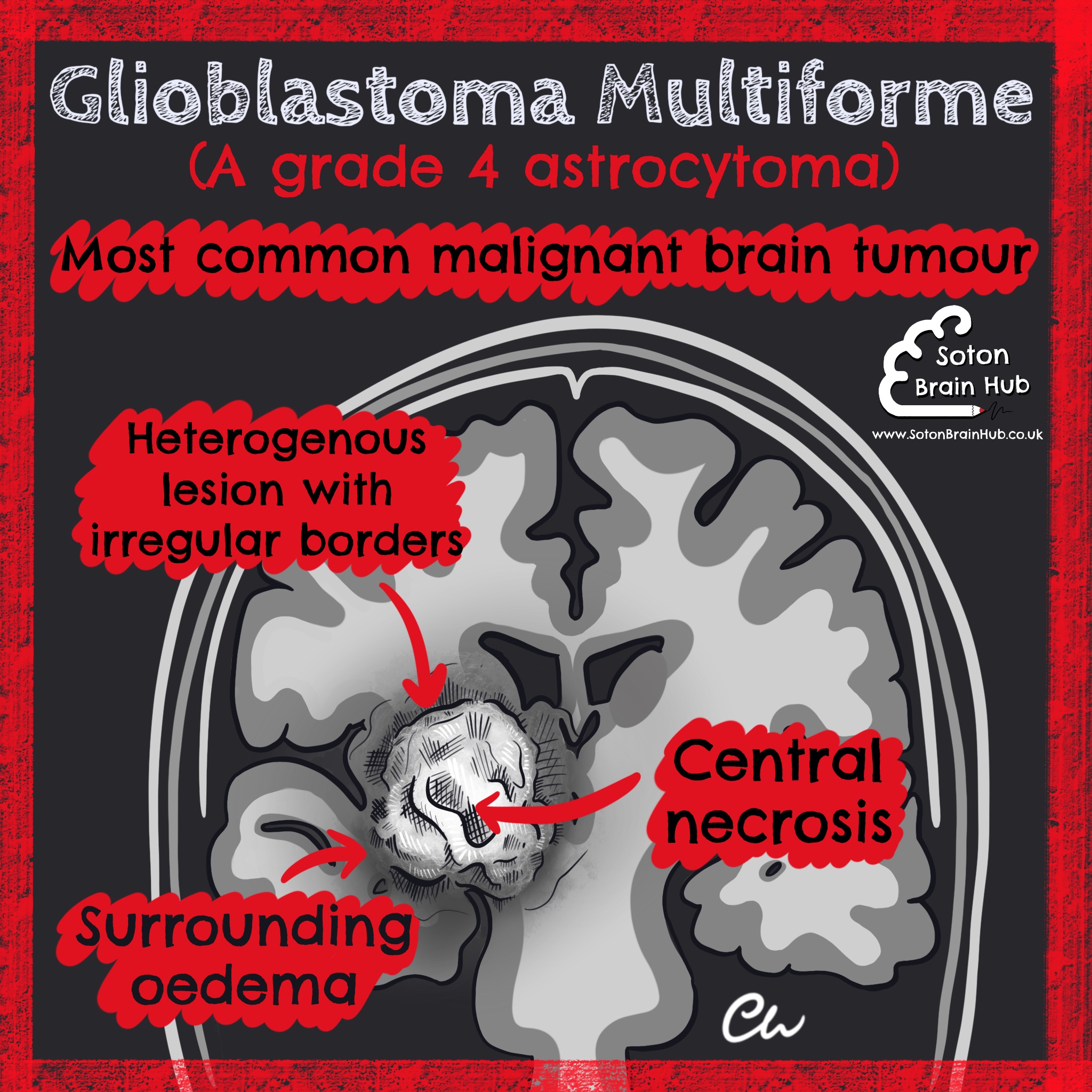
Symptoms vary and depend on the size and location of the tumour. They may include headache (due to raised intracranial pressure), nausea and vomiting, seizures and focal neurological symptoms (e.g. weakness, numbness, visual disturbance, speech problems).
Management depends on the size and location of the tumour, and the general health of the patient. Complete excision of the tumour is preferable but often difficult 
 . Adjuvant chemotherapy with temozolomide
. Adjuvant chemotherapy with temozolomide  and radiotherapy may also be used. Other options include biopsy and palliative care.
and radiotherapy may also be used. Other options include biopsy and palliative care.
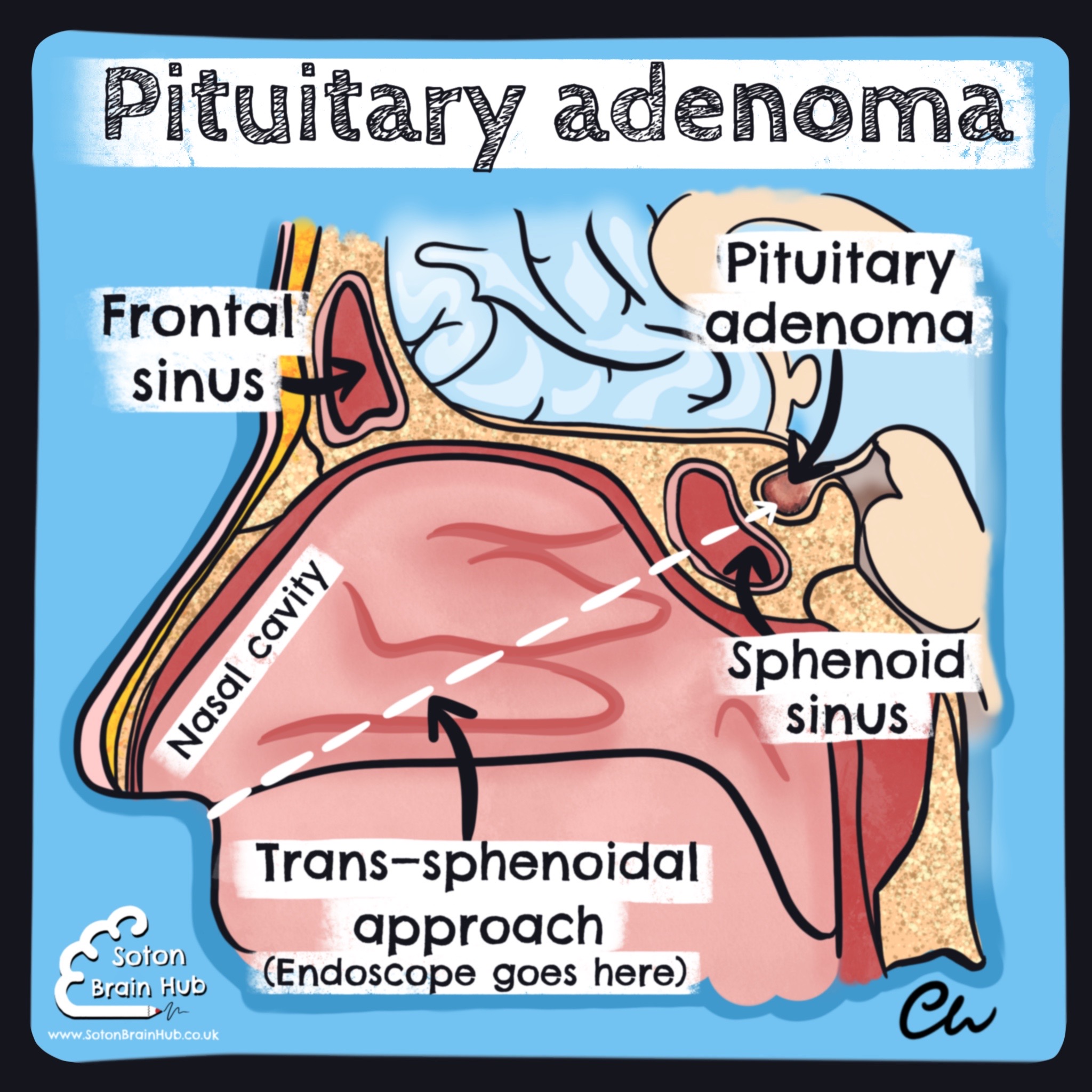
Pituitary adenomas are slow growing, benign tumours that arise in the anterior pituitary gland. They can be hormone secreting or non-hormone secreting.
Depending on the hormone secreted, pituitary adenomas can cause different symptoms: Prolactin secretion  low libido, amenorrhoea (in women), impotence (in men), galactorrhoea, infertility Growth hormone secretion acromegaly ACTH secretion Cushing’s disease
low libido, amenorrhoea (in women), impotence (in men), galactorrhoea, infertility Growth hormone secretion acromegaly ACTH secretion Cushing’s disease
Additionally, large pituitary adenomas (macroadenomas) may cause the classic bitemporal hemianopia (a favourite of exam questions!) due to suprasellar extension and compression of the optic chiasm. Rarely when a macroadenoma outgrows its blood supply, spontaneous haemorrhage and infarction can occur within it (pituitary apoplexy). This is a medical emergency! 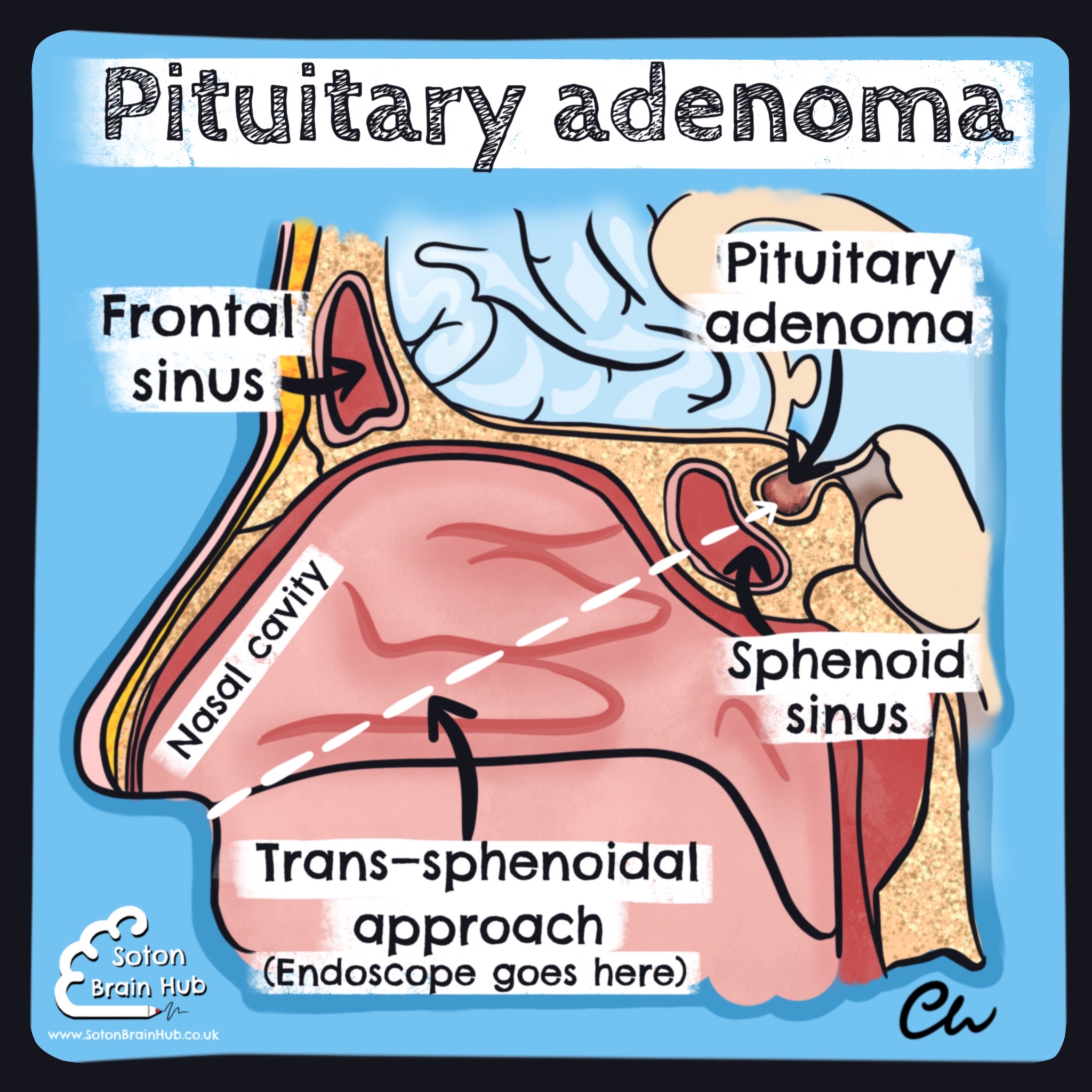
The primary treatment for most patients with secreting pituitary adenomas is surgical resection. This is typically an endoscopic endonasal trans-sphenoidal decompression.
The surgeon passes the endoscope through the nose and accesses the pituitary gland via the sphenoid sinus. This technique is popular as it is minimally invasive and avoids the need for a craniotomy.
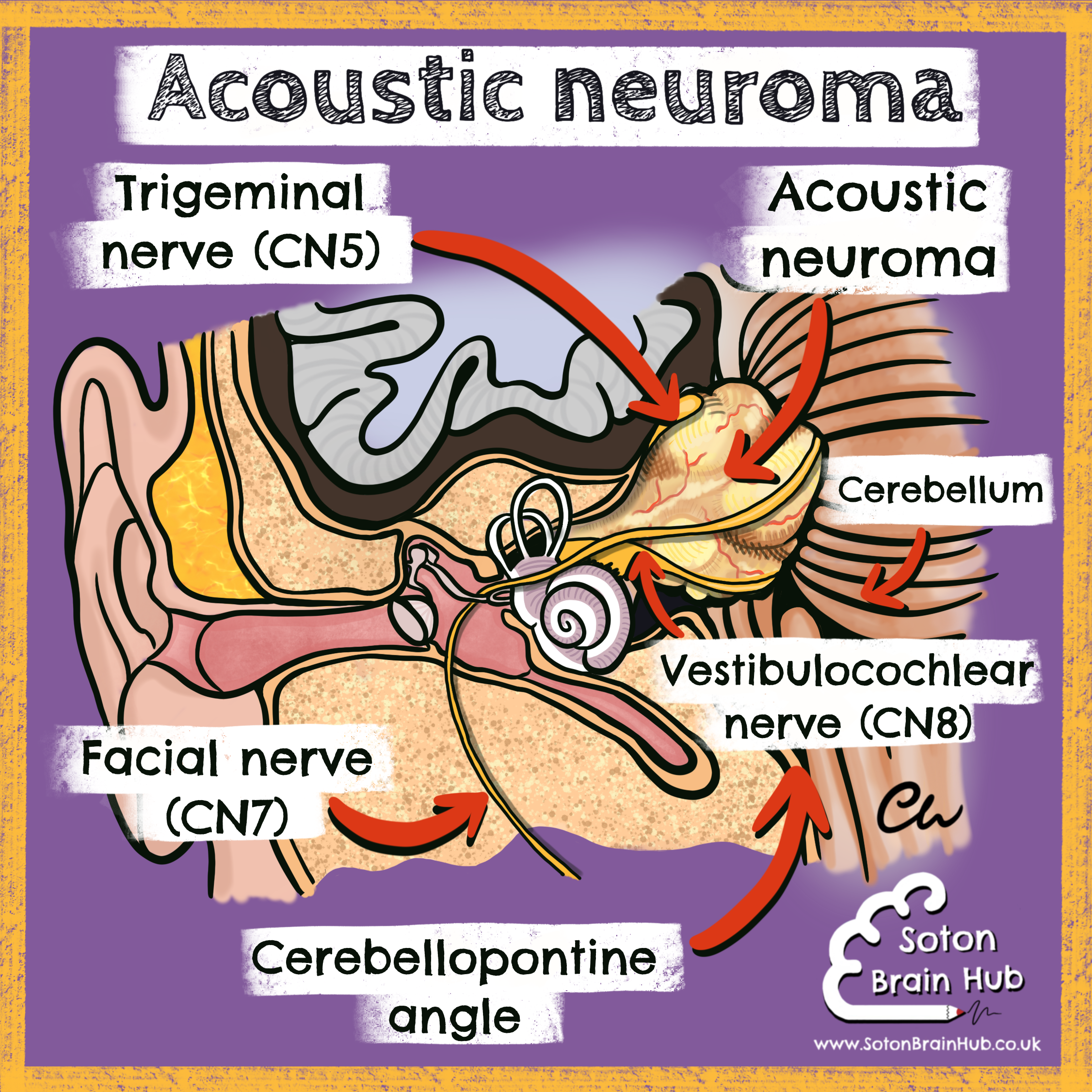
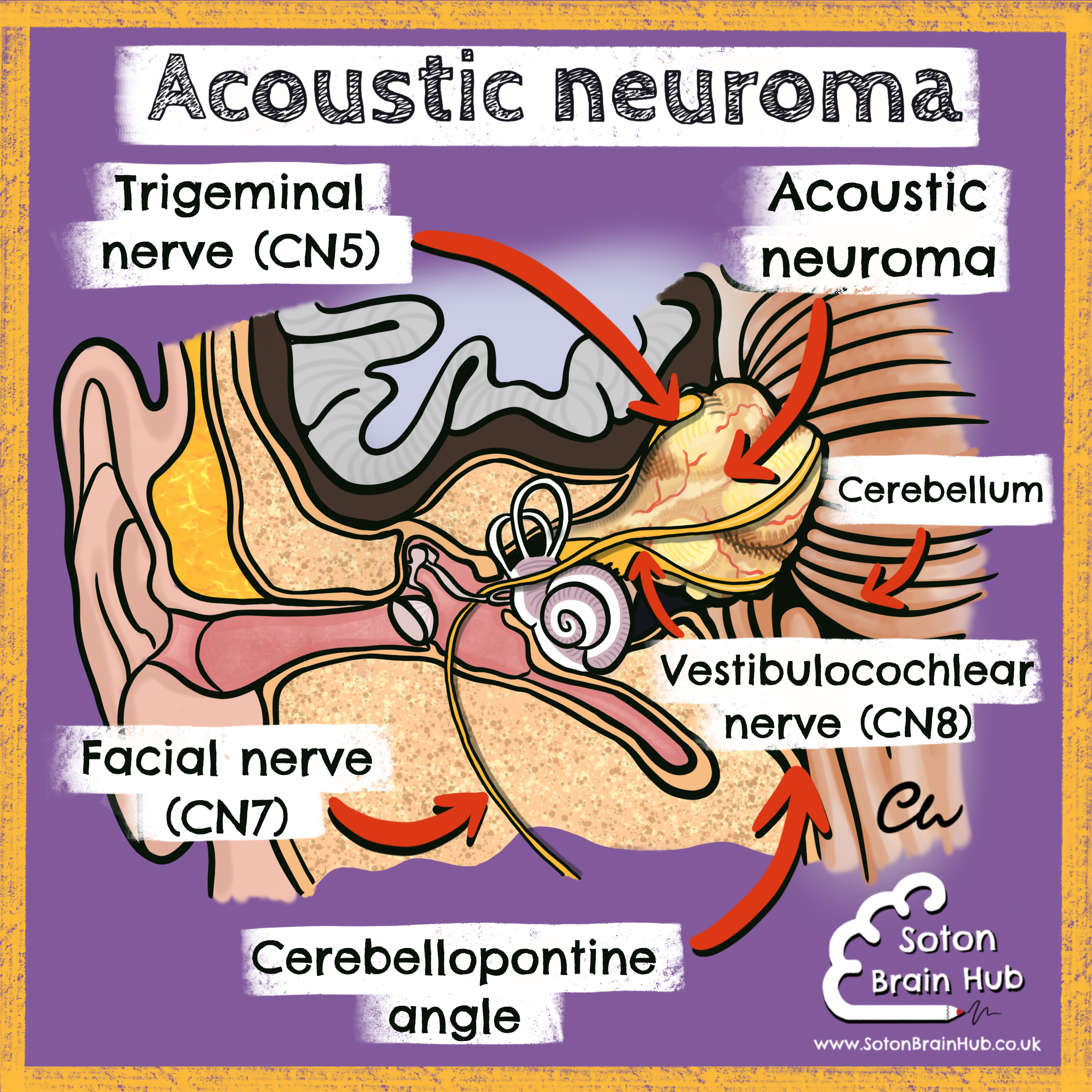
An acoustic neuroma (also known as a vestibular schwannoma) is benign tumour of the Schwann cells around the vestibulocochlear nerve (CN8).
They account for 5% of intracranial tumours and 90% of cerebellopontine angle tumours.
Bilateral vestibular schwannomas are seen in neurofibromatosis type .
Signs and symptoms of an acoustic neuroma depend on its size and the cranial nerves affected. They can be predicted when you know the anatomy.
 Features may include:
Features may include: Vestibulocochlear nerve (CN8): vertigoo
Vestibulocochlear nerve (CN8): vertigoo , unilateral sensorineural hearing loss, unilateral tinnitusTrigeminal nerve (CN5): absent corneal reflex, unilateral facial numbness, weakness of the muscles of mastication
, unilateral sensorineural hearing loss, unilateral tinnitusTrigeminal nerve (CN5): absent corneal reflex, unilateral facial numbness, weakness of the muscles of mastication Facial nerve (CN7): ipsilateral facial palsy
Facial nerve (CN7): ipsilateral facial palsy , hyperacusis (noise sensitivity), impaired lacrimation
, hyperacusis (noise sensitivity), impaired lacrimation , loss of taste of the anterior 2/3 of the tongue
, loss of taste of the anterior 2/3 of the tongue
A large acoustic neuroma could also affect the glossopharyngeal (CN9) and vagus (CN10) nerves, have mass effect on the cerebellum (ataxia, ipsilateral cerebellar syndrome) and the brainstem, and cause hydrocephalus.
Management may be observation, radiotherapy or surgical resection.
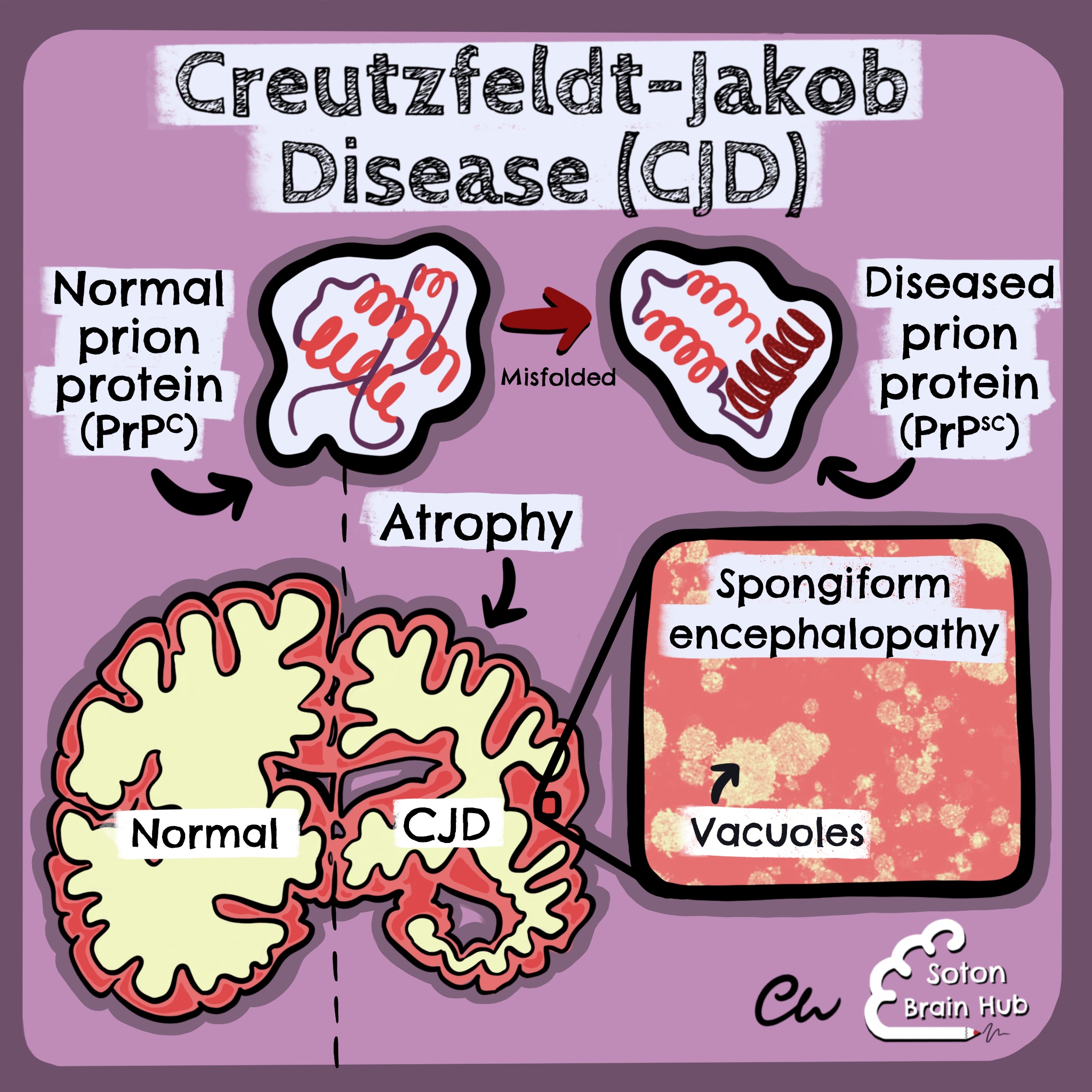
Creutzfeldt-Jakob disease (CJD) is a very rare and fatal degenerative brain disorder. CJD is a type of prion disease, which is caused by an infectious protein known as a prion.
A prion protein is a normal structural component of the nervous system . However, it can become misfolded. This alters its tertiary structure but its amino acid sequence remains the same. A misfolded prion protein can catalyse the conversion of other normal prion proteins (PrPc) into abnormal ones (PrPsc) in a chain reaction  . These abnormal prion proteins accumulate in the brain causing irreversible damage.
. These abnormal prion proteins accumulate in the brain causing irreversible damage.
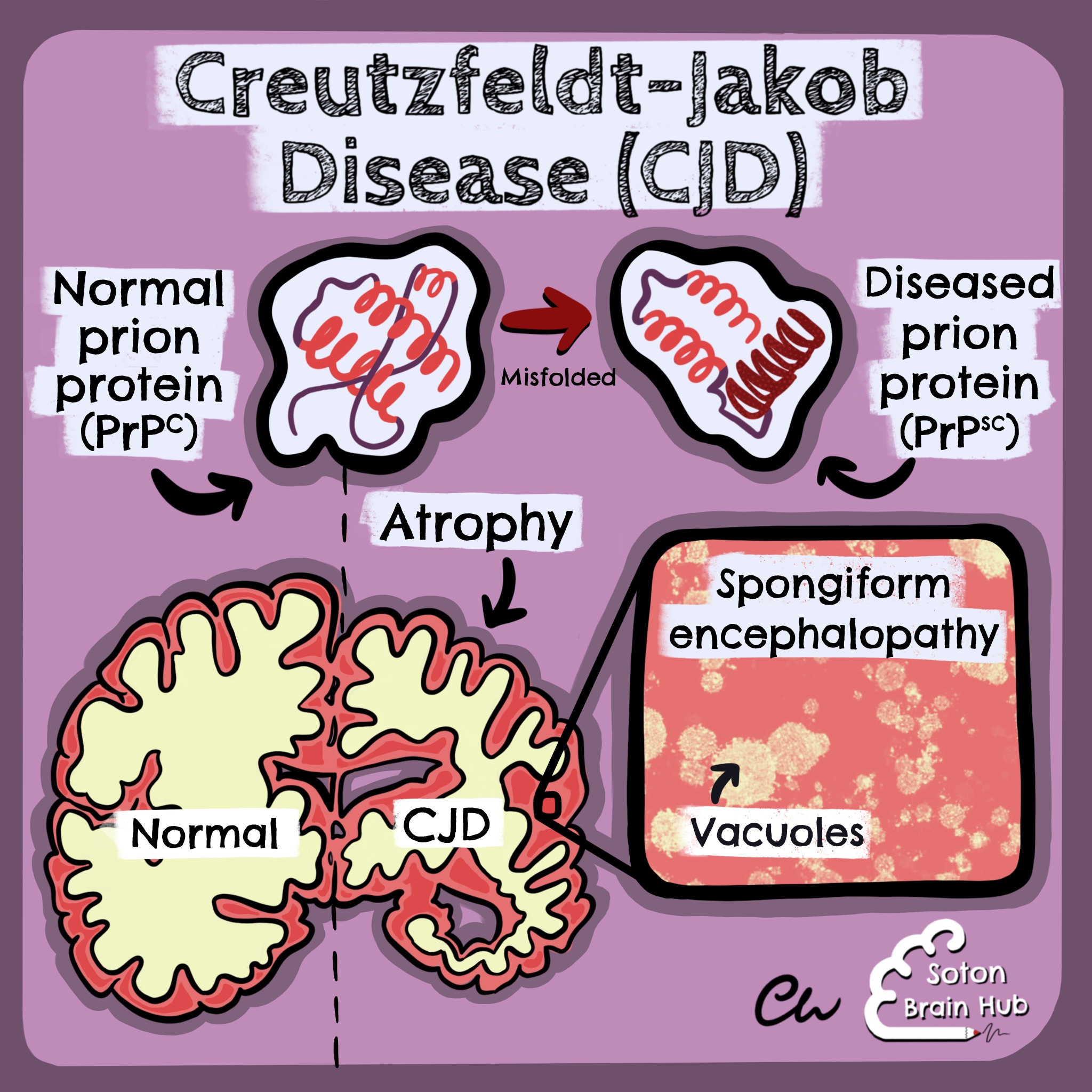 This causes vacuolation in the grey matter of the brain and results in a spongy appearance histologically
This causes vacuolation in the grey matter of the brain and results in a spongy appearance histologically  . It is known as spongiform encephalopathy.
. It is known as spongiform encephalopathy.
CJD can be sporadic (most common), acquired (variant CJD), familial
(most common), acquired (variant CJD), familial  (due to a mutation in the PRNP gene) or iatrogenic (e.g. from a contaminated corneal transplant or blood transfusion
(due to a mutation in the PRNP gene) or iatrogenic (e.g. from a contaminated corneal transplant or blood transfusion ). Variant CJD is caused by consuminginfected material, such as beef
). Variant CJD is caused by consuminginfected material, such as beef  from a cow with bovine spongiform encephalopathy - also known as ‘Mad Cow Disease’
from a cow with bovine spongiform encephalopathy - also known as ‘Mad Cow Disease’ .
.
Symptoms are often rapidly progressive and can include ataxia, slurred speech, involuntary movements (myoclonus), muscle weakness, visual disturbance, behavioural change and dementia.The definitive diagnosis is via brain biopsy  (usually post mortem).There is no available treatment and most patients die within 1 year of symptom onset.
(usually post mortem).There is no available treatment and most patients die within 1 year of symptom onset.
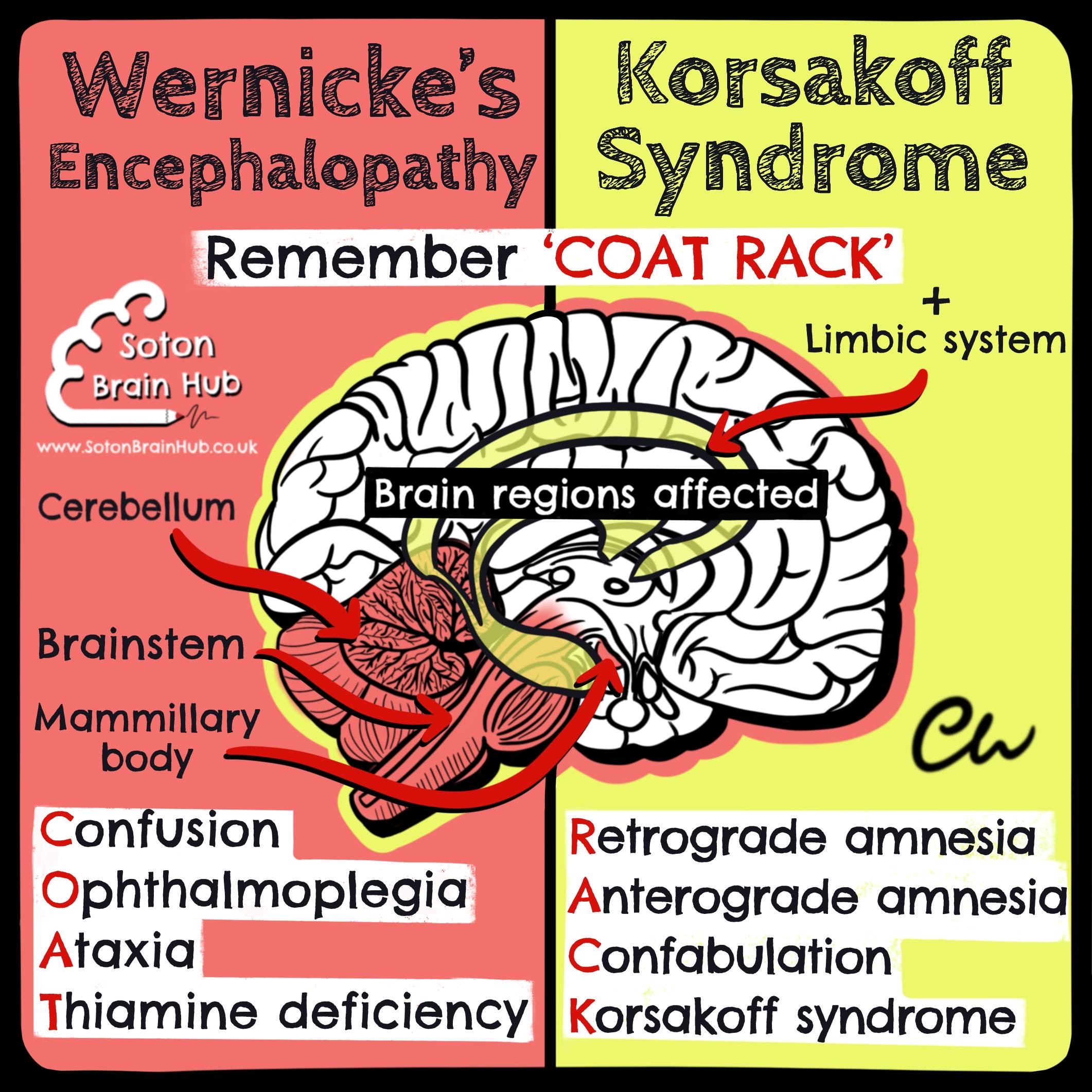
Wernicke-Korsakoff syndrome is a spectrum of disease resulting from thiamine (vitamin B1) deficiency. It is associated with chronic alcohol consumption  . Thiamine is required for the glycolytic pathway of carbohydrate metabolism.
. Thiamine is required for the glycolytic pathway of carbohydrate metabolism.
Patients with alcohol dependence may be deficient in thiamine for multiple reasons, including inadequate thiamine intake (due to poor diet, malnutrition and anorexia), reduced thiamine absorption and reduced storage (due to liver damage). 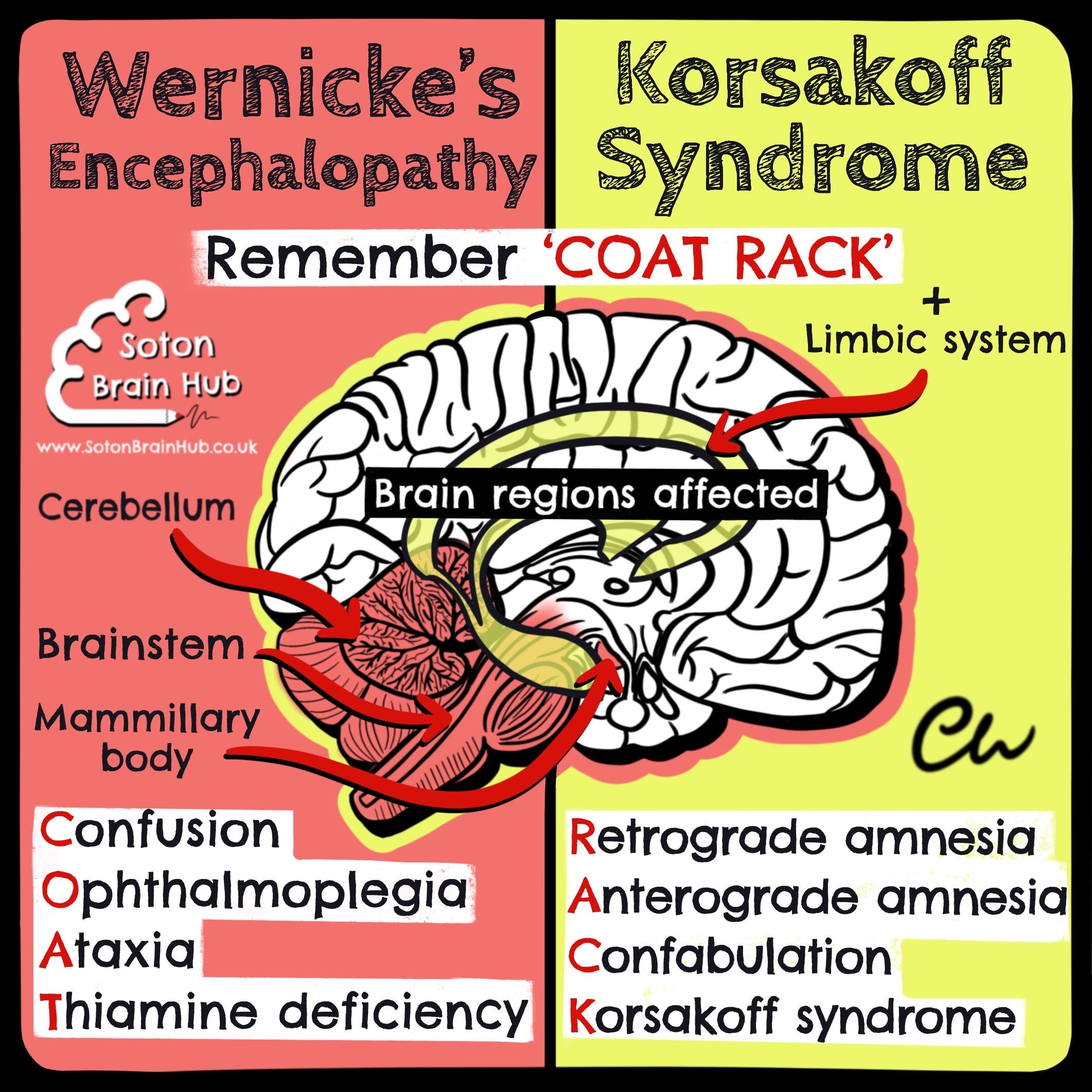
Wernicke’s encephalopathy is the acute and reversible stage of the disease  . It is a medical emergency
. It is a medical emergency . The classical triad is confusion, ophthalmoplegia and ataxia
. The classical triad is confusion, ophthalmoplegia and ataxia . However the triad is only seen in around 10% of patients so it is important to have a high level of suspicion. It affects the cerebellum, brainstem and mammillary body .
. However the triad is only seen in around 10% of patients so it is important to have a high level of suspicion. It affects the cerebellum, brainstem and mammillary body .
Wernicke’s encephalopathy can progress to Korsakoff syndrome, which is the chronic and irreversible stage of the disease. Clinical features of Korsakoff syndrome include profound memory impairment  with anterograde and retrograde amnesia (due to effects on the limbic system) and confabulation . Treatment is with thiamine replacement.
with anterograde and retrograde amnesia (due to effects on the limbic system) and confabulation . Treatment is with thiamine replacement.
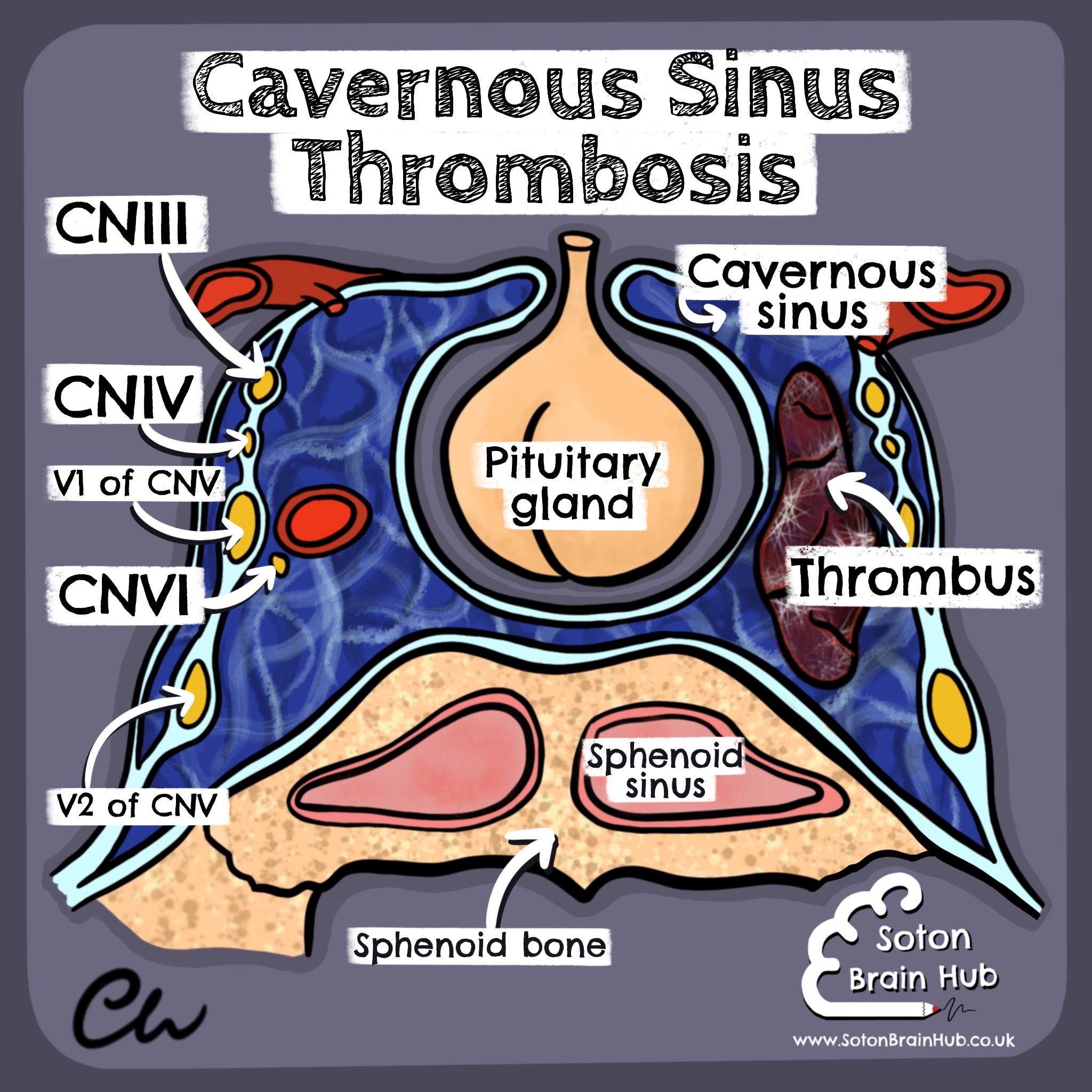
Cavernous sinus thrombosis is the formation of a blood clot (or thrombus)🩸within the cavernous sinus (one of the dural venous sinuses at the base of the brain) 🧠. It is usually caused by an extra-cranial infection that spreads (e.g from the paranasal sinuses or face). Staphylococcus aureus is typically the associated organism🔬🧫. Signs and symptoms of cavernous sinus thrombosis may include:
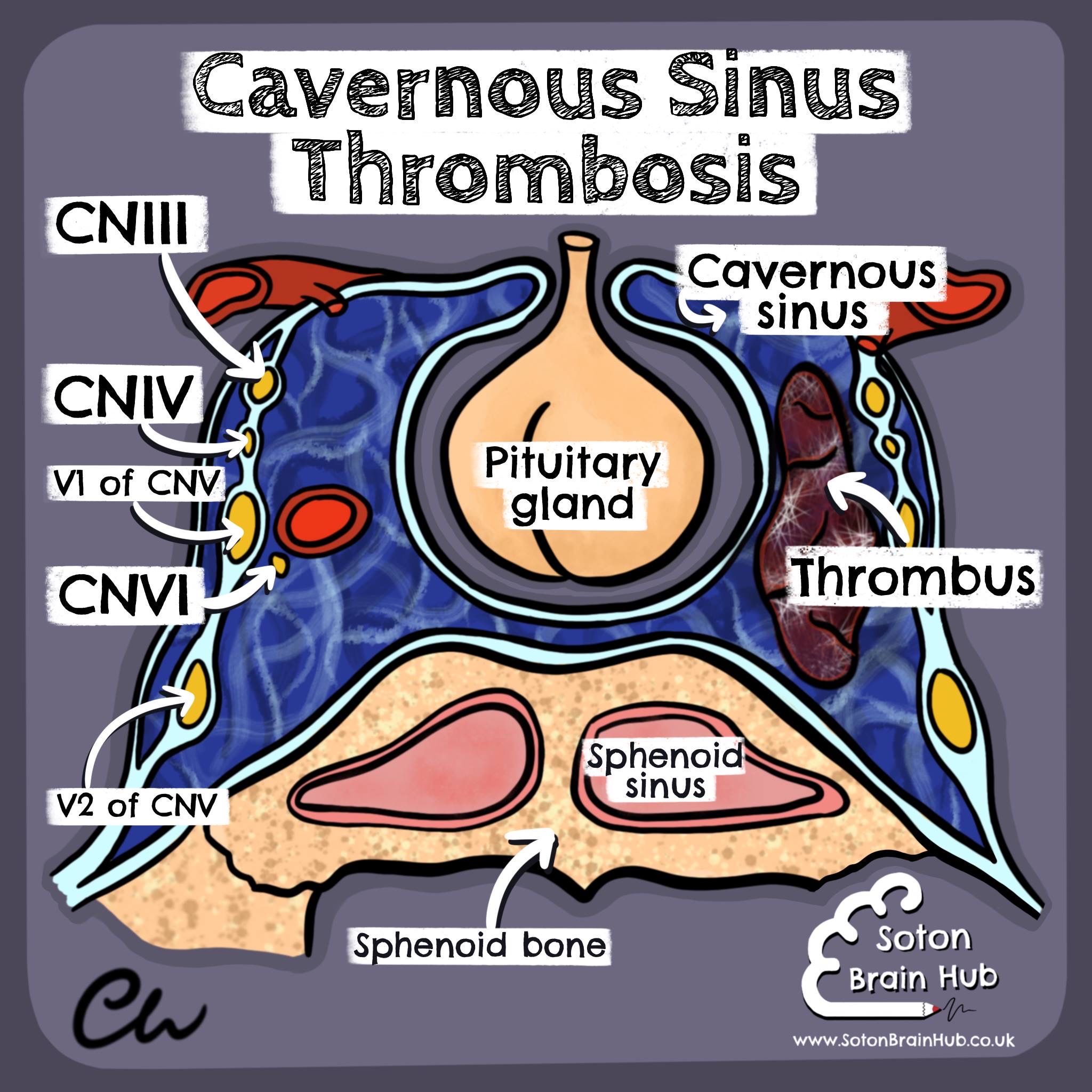 Severe headache🤯, periorbital oedema, proptosis, photophobia 👁 and palsies of the cranial nerves that traverse the cavernous sinus.
Severe headache🤯, periorbital oedema, proptosis, photophobia 👁 and palsies of the cranial nerves that traverse the cavernous sinus.
Damage to the abducens nerve (CNVI) often occurs first, due to its location within the cavernous sinus. Along with damage to the oculomotor (CNIII) and trochlear (CNIV) nerves, this can result in painful ophthalmoplegia and diplopia 👀.
Additionally, damage to the ophthalmic (V1) and maxillary (V2) divisions of the trigeminal nerve (CNV) can result in facial pain🤦, paraesthesia and an impaired corneal reflex.
This infection is life threatening and requires immediate treatment with antibiotics 💊
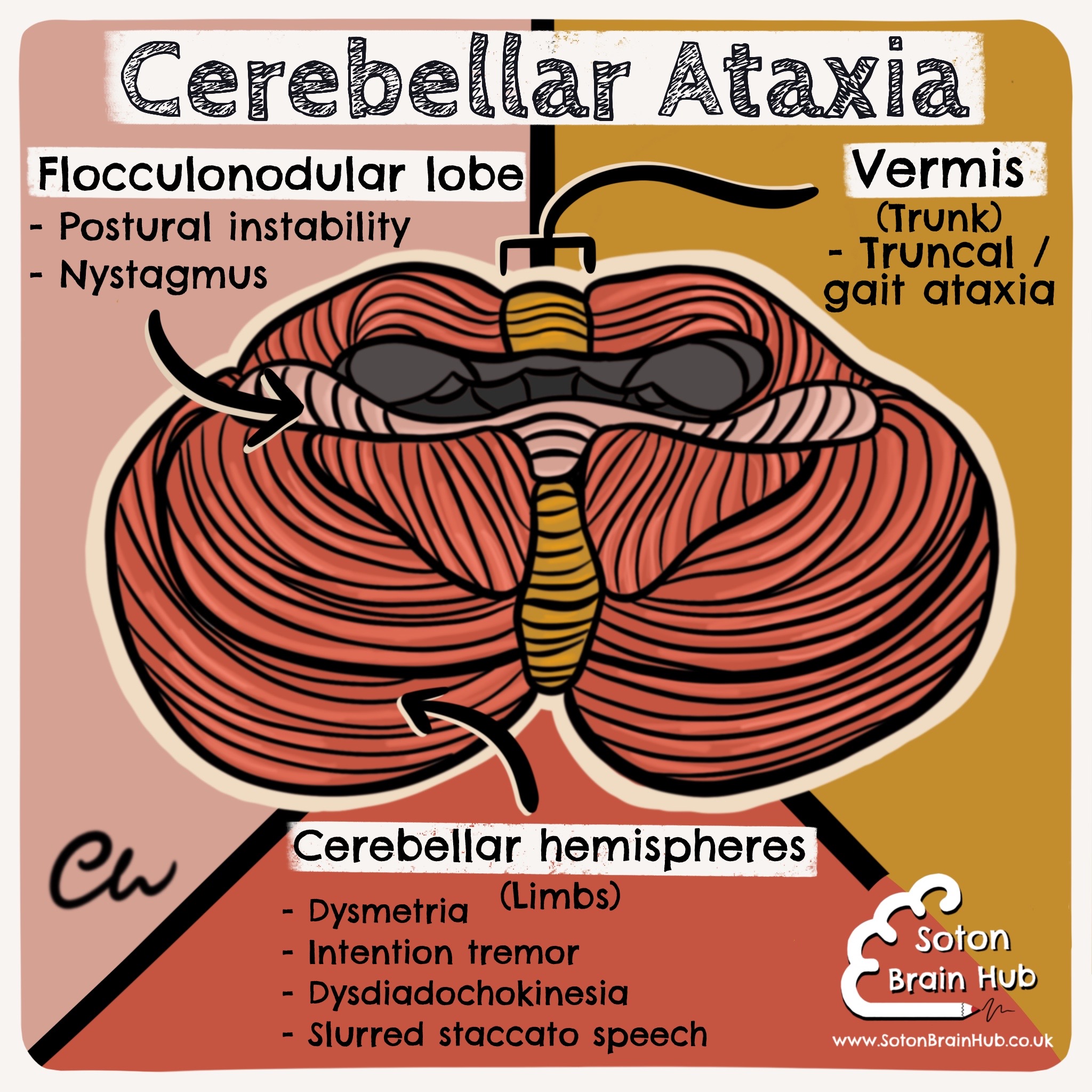
Ataxia is a term for a group of disorders that affect coordination, balance and speech. Cerebellar ataxia is ataxia caused by dysfunction of the cerebellum 🧠. It can be acquired (e.g. due to trauma, stroke, brain tumours, chronic alcohol misuse, multiple sclerosis and vitamin B12 deficiency) or hereditary 🧬 (e.g. Friedreich’s ataxia and spinocerebellar ataxias). Like the cerebrum, the cerebellum has a somatotopic organisation 🗺.
Damage to different areas of the cerebellum can result in different signs. The central vermis corresponds to control of the trunk. Damage here can cause gait and truncal ataxia, which results in an ataxic broad based gait (best seen when heel-to-toe walking) 🧑🦯 and instability of the trunk when sitting.
The cerebellar hemispheres correspond to control of the limbs. Damage here can cause problems with voluntary limb movement, including dysmetria (past pointing with finger to nose testing 👈 and overshooting with the heel to shin test🦵), intention tremor 👋 (a tremor that only occurs during movement, and is worse towards the end phase).
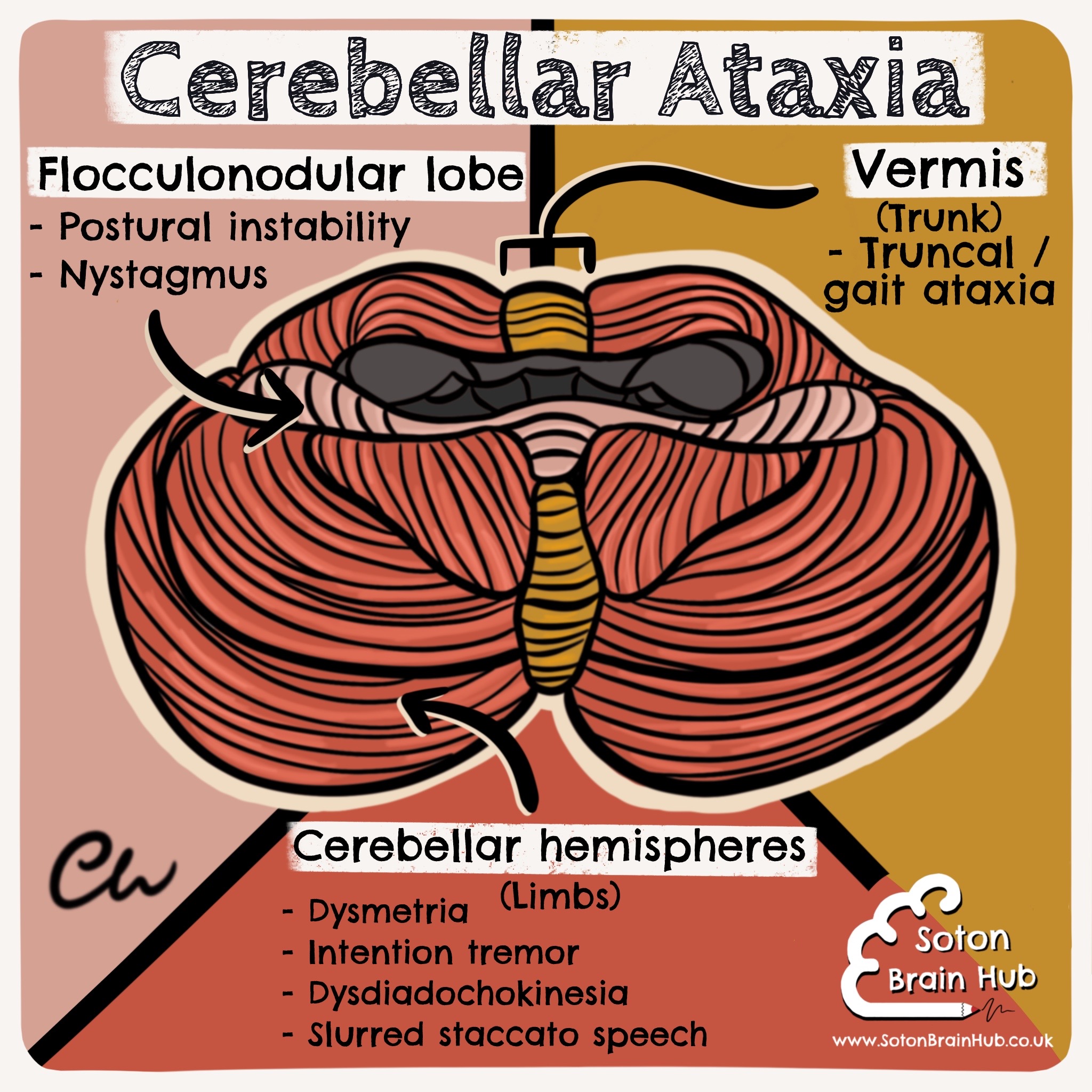
In addition dysdiadochokinesia can occur (an impaired ability to perform rapid alternating movements, that is best seen with alternating pronation and supination 🙏🏻).
It can also cause slurred staccato speech 🗣. Damage to the flocculonodular lobe results in postural instability and nystagmus (involuntary eye movements) 👀.
When cerebellar ataxia is suspected, it is important to perform Romberg’s test to rule out sensory ataxia (a problem with proprioception or vestibular function👂, rather than cerebellar function).
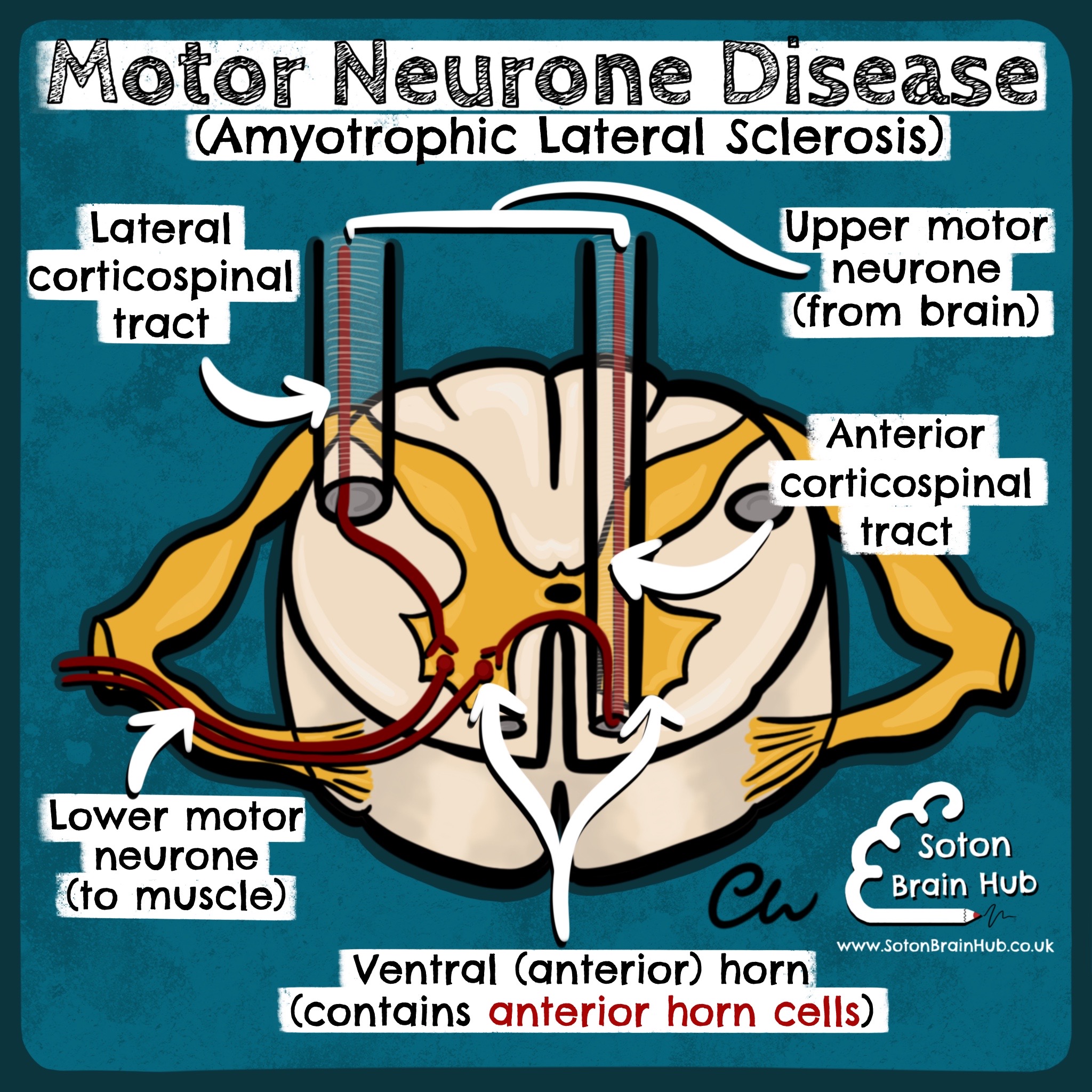
Motor neurone disease (MND) is a rare neurodegenerative disorder 🧠. There are various patterns of disease. The most common type is amyotrophic lateral sclerosis (ALS).
This typically presents with a combination of:
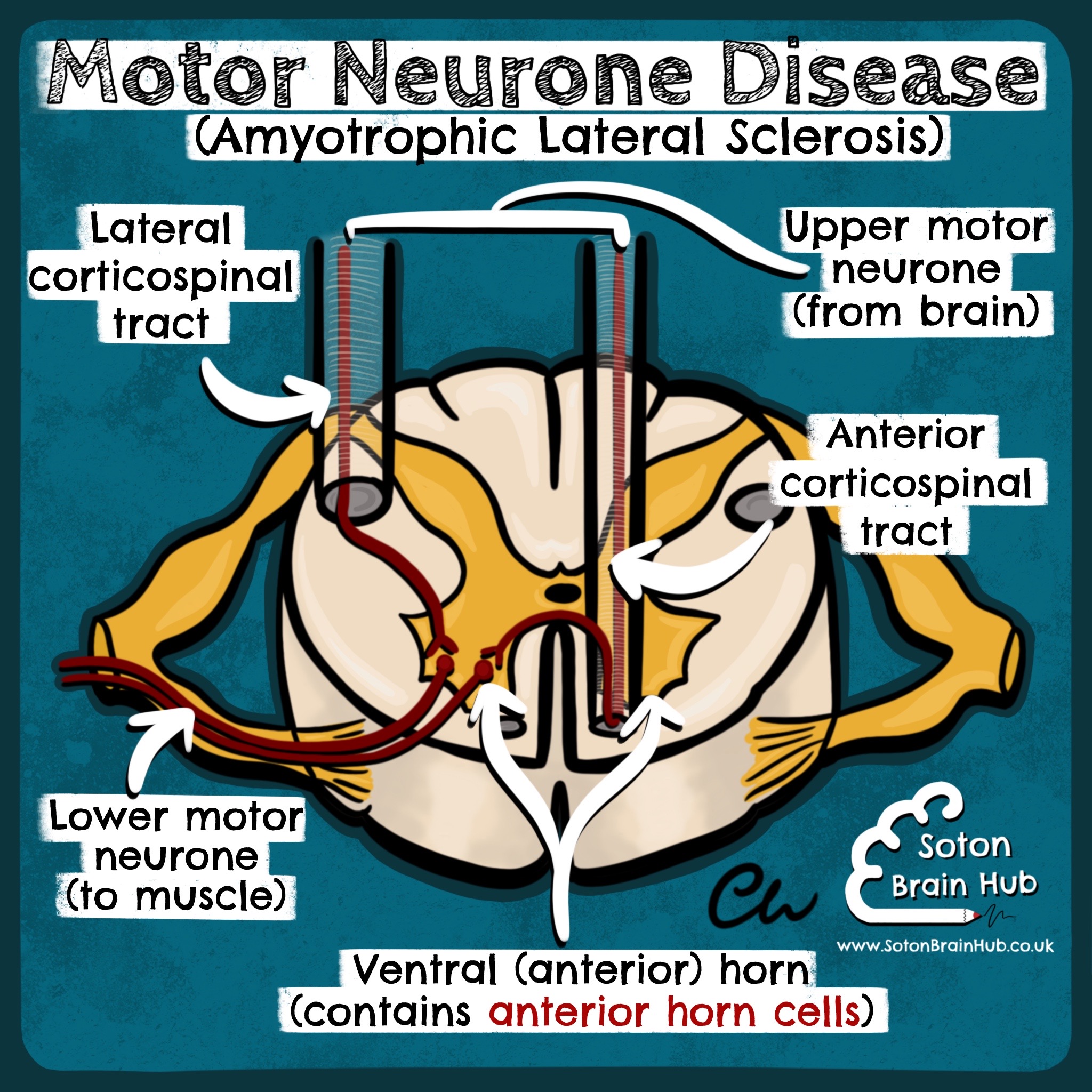 Upper motor neurone (UMN) ⬆️ and lower motor neurone (LMN) ⬇️ signs, as it affects the anterior horn cells and the corticospinal tracts.
Upper motor neurone (UMN) ⬆️ and lower motor neurone (LMN) ⬇️ signs, as it affects the anterior horn cells and the corticospinal tracts.
UMN signs can include hyperreflexia, hypertonia and spasticity. LMN signs can include fasciculations (e.g. of the tongue👅) and muscle atrophy (particularly of the tibialis anterior🦵 and the small muscles of the hand✋)
Other patterns of MND affect purely UMN (e.g. primary lateral sclerosis) or LMN (e.g. progressive muscular atrophy).
There may also be bulbar involvement (e.g. progressive bulbar palsy), resulting in dysarthria and dysphagia🗣.
Life expectancy is usually 2 to 5 years from the onset of symptoms.
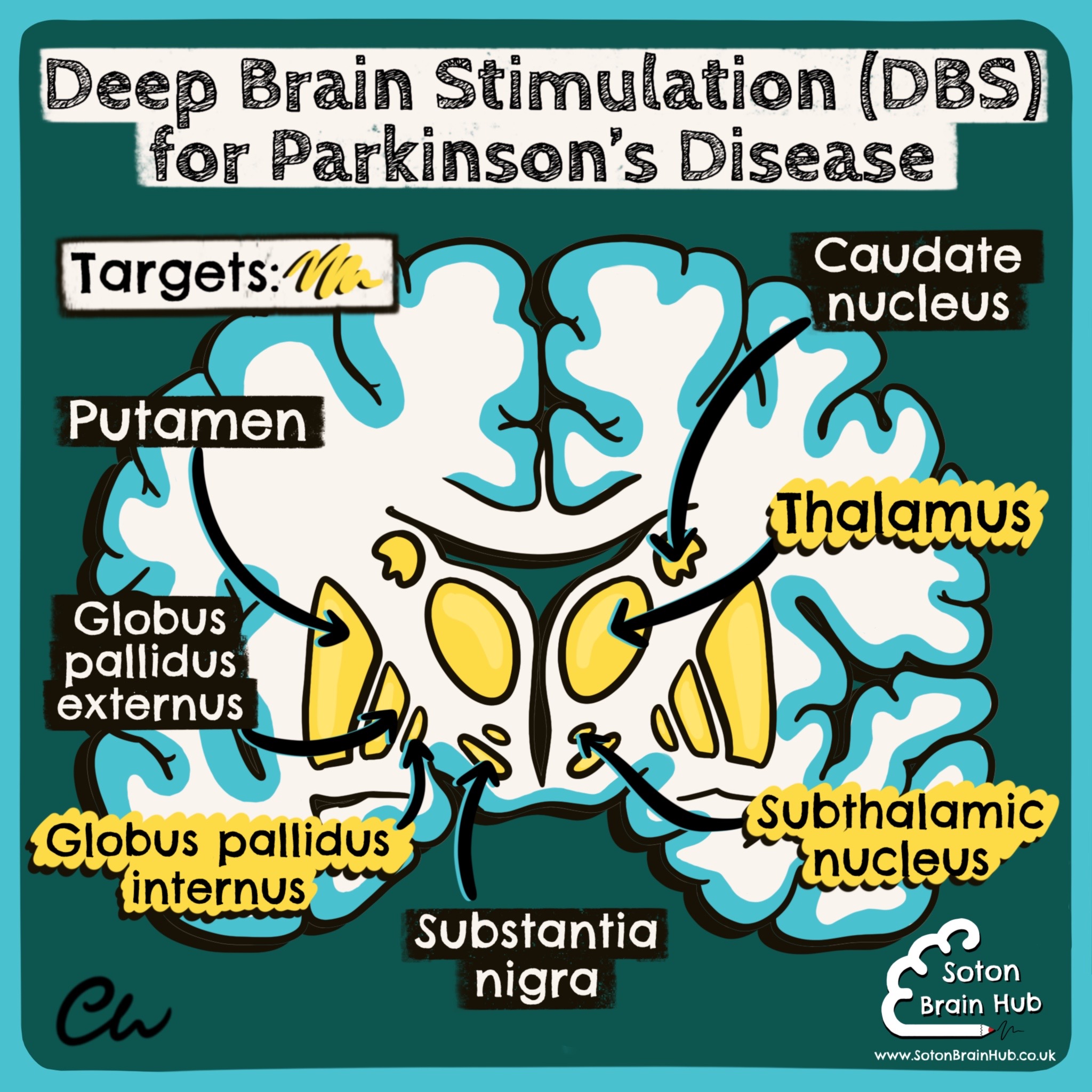
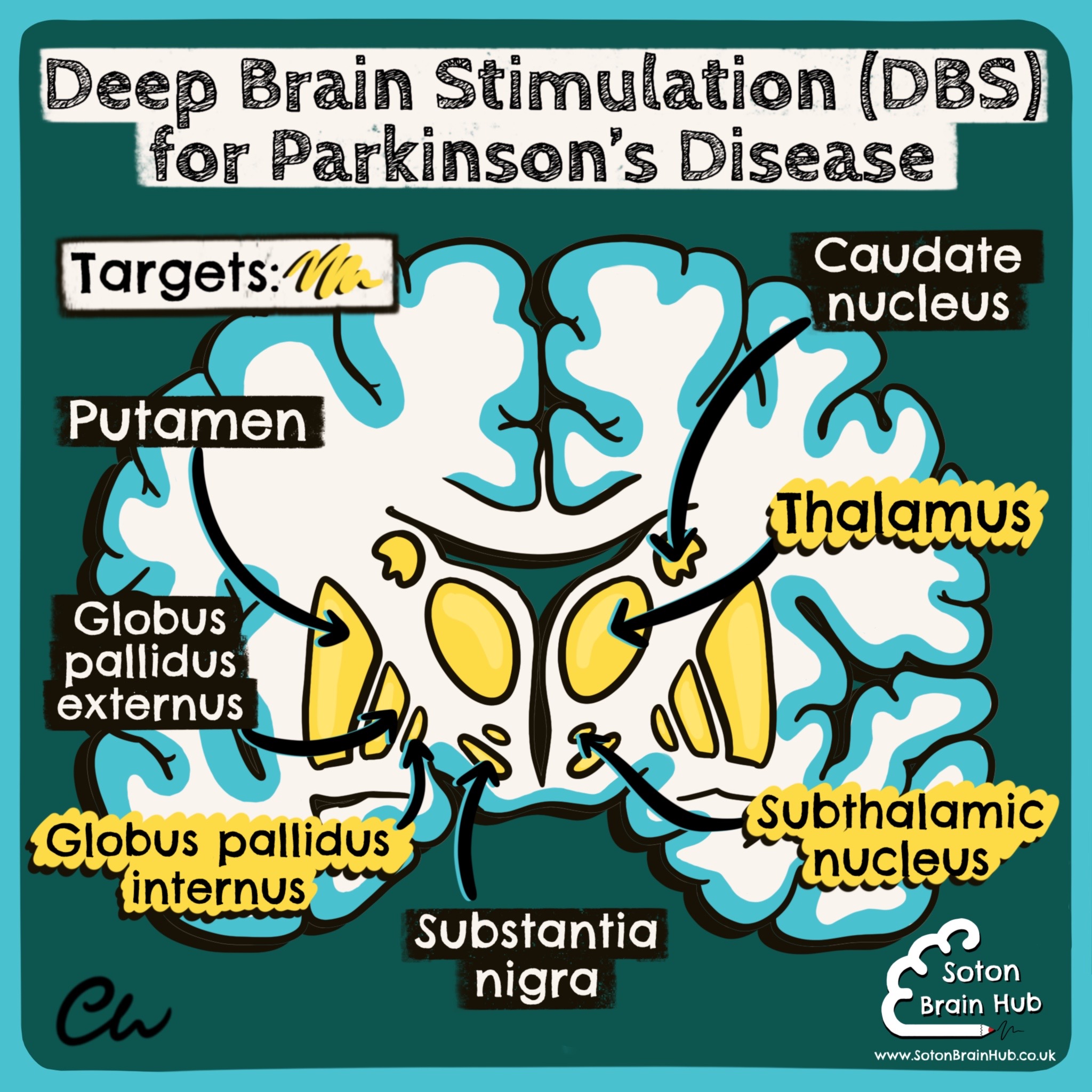
Deep brain stimulation (DBS) 🧠 may be an option for some patients with Parkinson’s Disease (PD) whose symptoms are no longer controlled with medication 💊. It is not curative and does not prevent progression of the disease 📈, however it can provide symptomatic relief for some patients. It is not suitable for all patients with PD. It involves delivering high frequency stimulation 💥 from an implantable pulse generator to specific areas in the basal ganglia 🧠. This alters electrical signalling through these areas and can result in smoother movement and improve motor fluctuations 🚶♂️
 🔴 Motor symptoms that previously responded well to medication before surgery are the most likely to improve with DBS.
🔴 Motor symptoms that previously responded well to medication before surgery are the most likely to improve with DBS.
🔴 DBS of the globus pallidus internus may reduce tremor, rigidity, bradykinesia, gait problems and dyskinesia 👋.
🔴 DBS of the thalamus can improve tremor, but not other motor symptoms of PD. DBS of the subthalamic nucleus can reduce all motor symptoms.
However, it is often avoided in patients with a history of cognitive or mood problems (e.g. depression) 🌨 as it may exacerbate these.
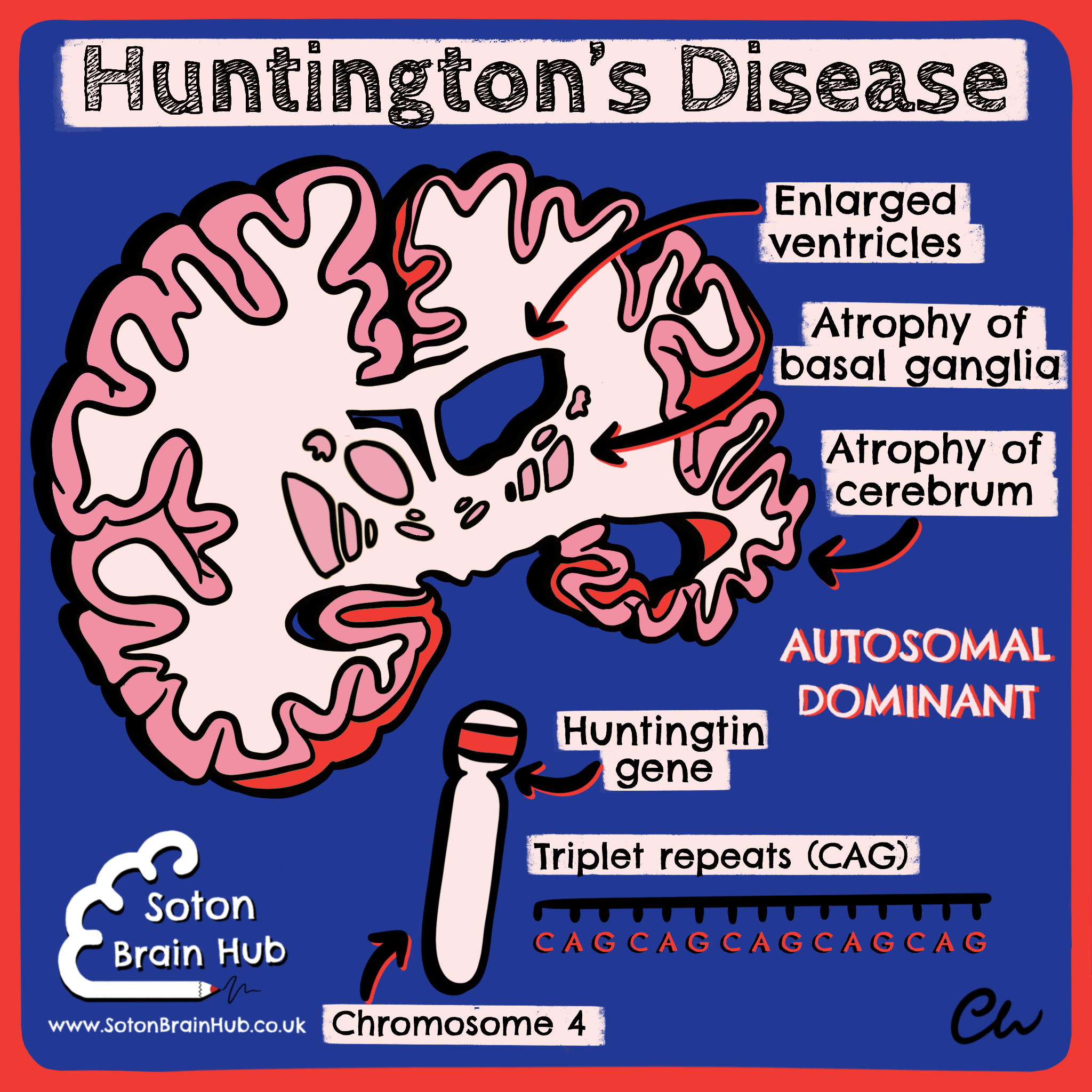
⭕️ Huntington's disease is a rare inherited neurodegenerative disorder 🧠. It is characterised by the development
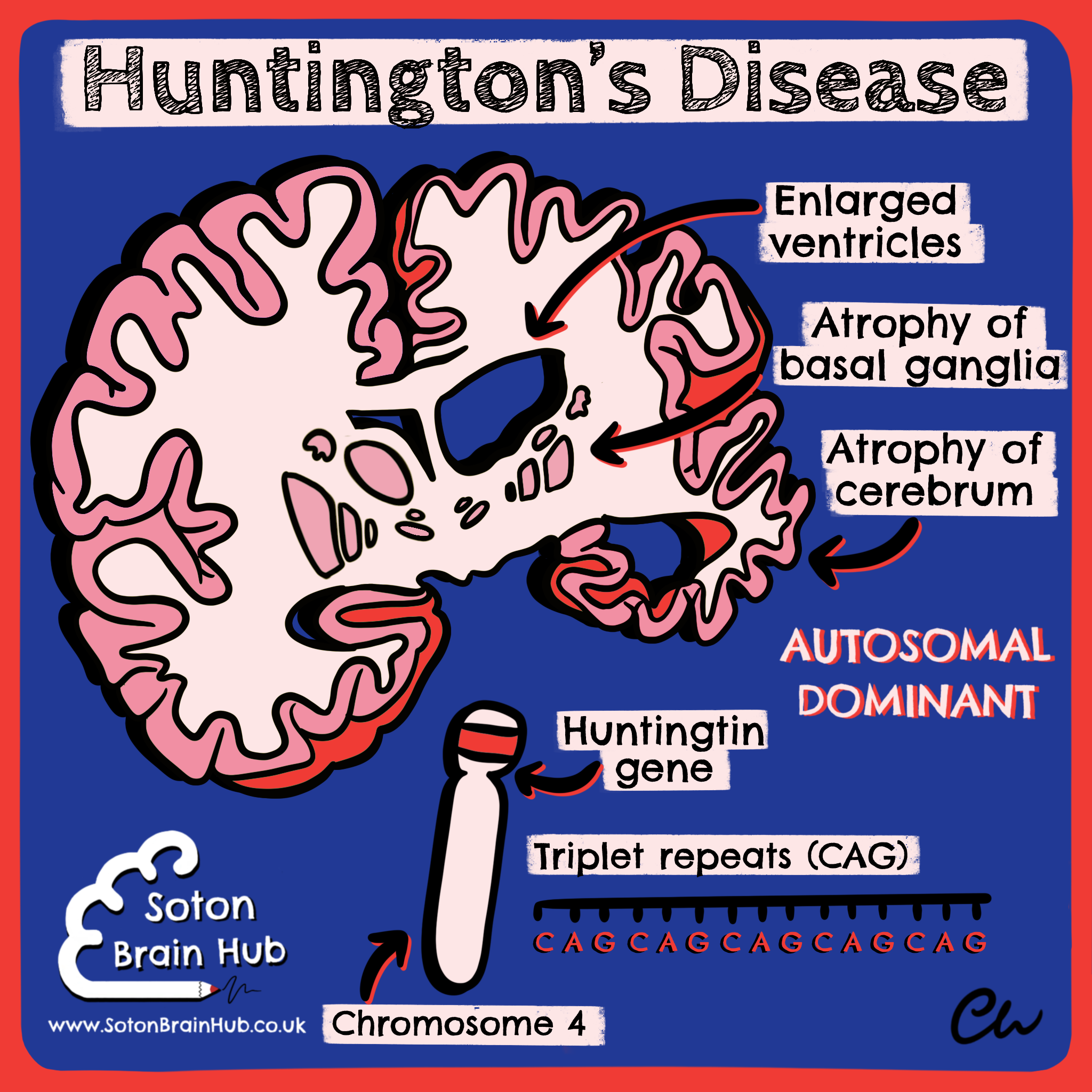 of involuntary muscle movements (including chorea and athetosis)👋, dystonia, cognitive decline, personality change (irritability and apathy😠) and dementia.
of involuntary muscle movements (including chorea and athetosis)👋, dystonia, cognitive decline, personality change (irritability and apathy😠) and dementia.
☑️ It is progressive and incurable. It is an autosomal dominant condition caused by a defect in the Huntingtin gene on chromosome 4🧬. It is known as a trinucleotide repeat disorder as there is a repeat expansion of the base sequence CAG (over 35 times).
☑️ This unstable gene results in nerve degeneration which causes atrophy of the brain and basal ganglia (particularly the caudate nucleus). Anticipation is seen in Huntington’s Disease, where successive generations have earlier symptom onset, due to an increasing number of CAG repeats📈.
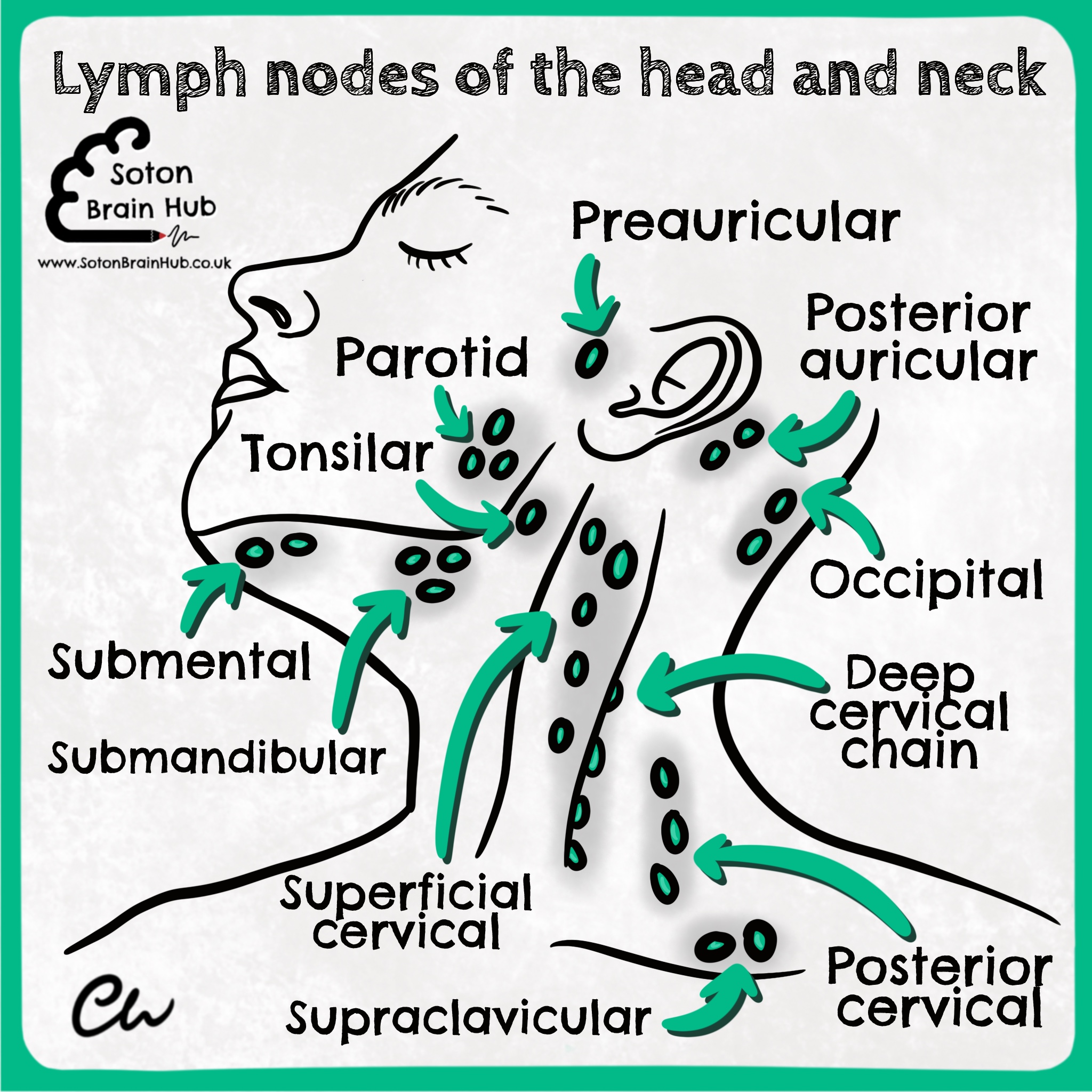
The lymphatic system of the head and neck consists of a number of regional superficial cervical lymph nodes and a deep cervical group.
🔴 Lymph from the superficial tissues passes through the superficial lymph nodes and drains to the deep cervical lymph nodes close to the internal jugular veins.
🔴 The final pathway for all the lymph of the head and neck are the jugular trunks. On the left the trunk opens into the thoracic duct and on the right into the right lymphatic duct.
The superficial groups of lymph nodes are situated at the junction of the head with
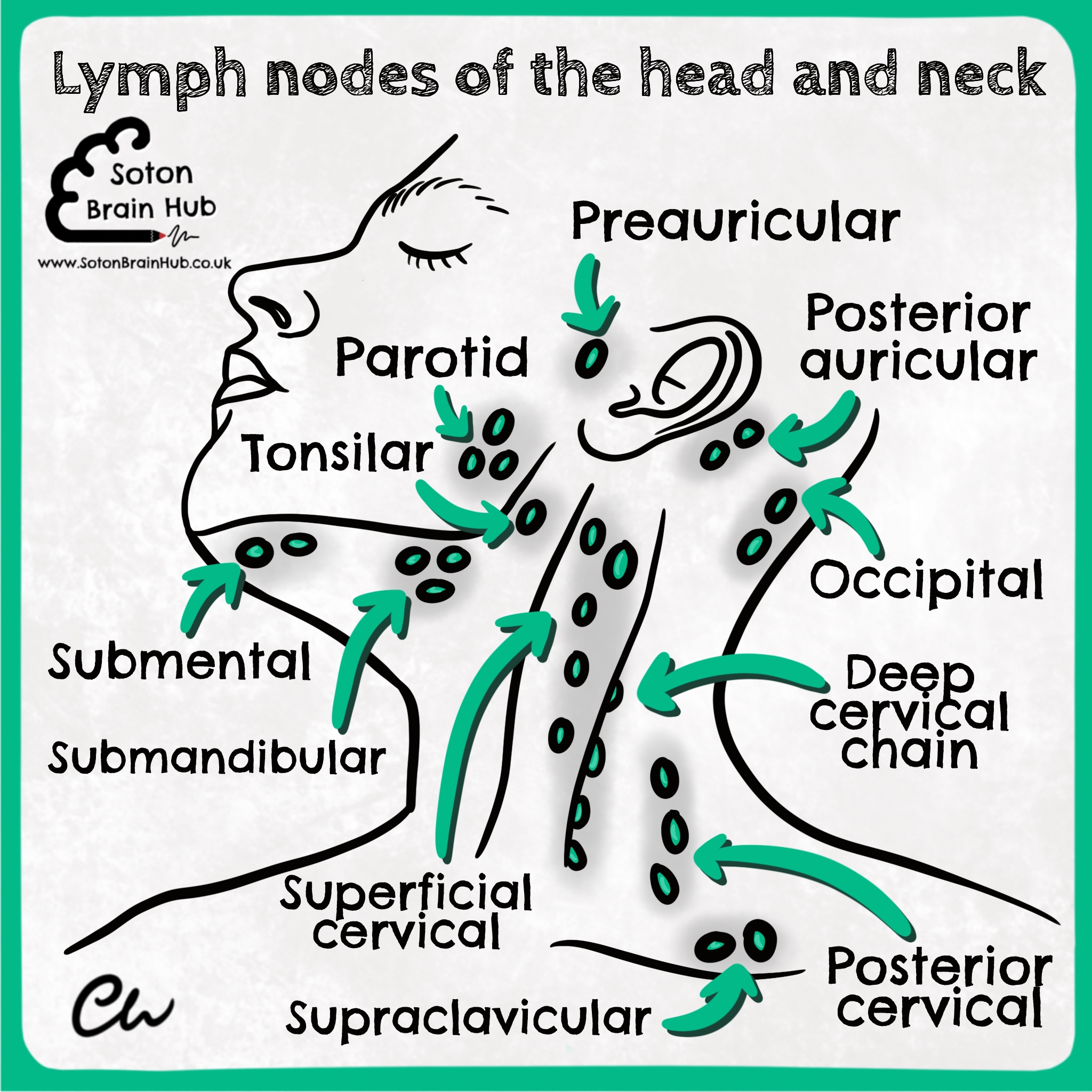
the neck, and five groups are worth remembering.
🔵 occipital
🔵 posterior auricular (mastoid)
🔵 preauricular (parotid)
🔵 submandibular
🔵 submental
The lymph nodes in the neck are examined from behind. The superficial and deep groups of nodes should be examined in a definite order so that none are omitted. Cervical lymphadenopathy is very common; careful clinical examination is required to establish the site of primary local or systemic infection or malignancy. When malignant disease of the face, lip, tongue, and the floor of the mouth has spread to the regional lymph nodes, those nodes may be removed.
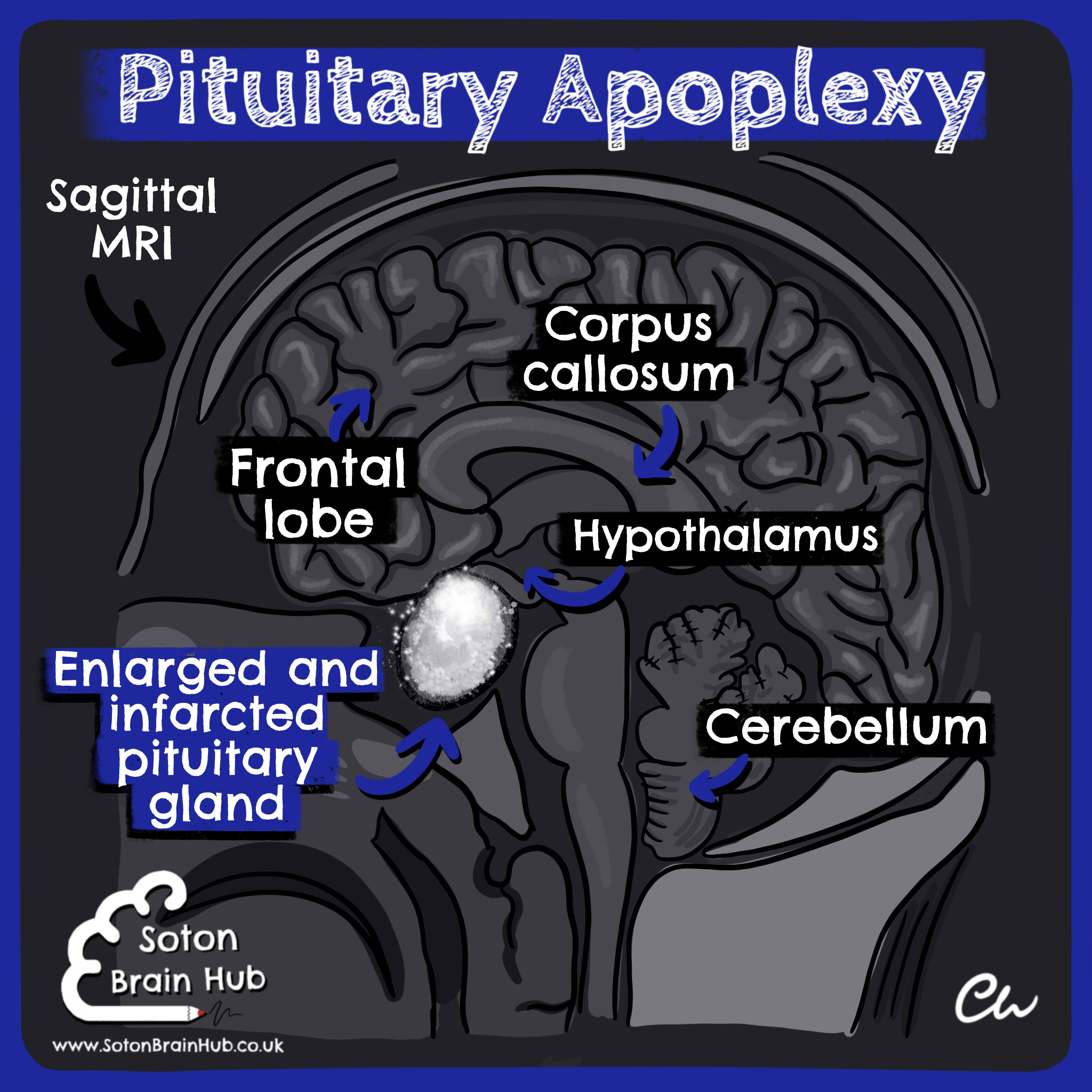
Pituitary apoplexy is a rare endocrine emergency ‼️ caused by necrosis of the pituitary gland 🧠. It mostly occurs due to a bleed 🩸from a pre-existing pituitary macro-adenoma. It may be the first presentation of the underlying tumour.
Another less common cau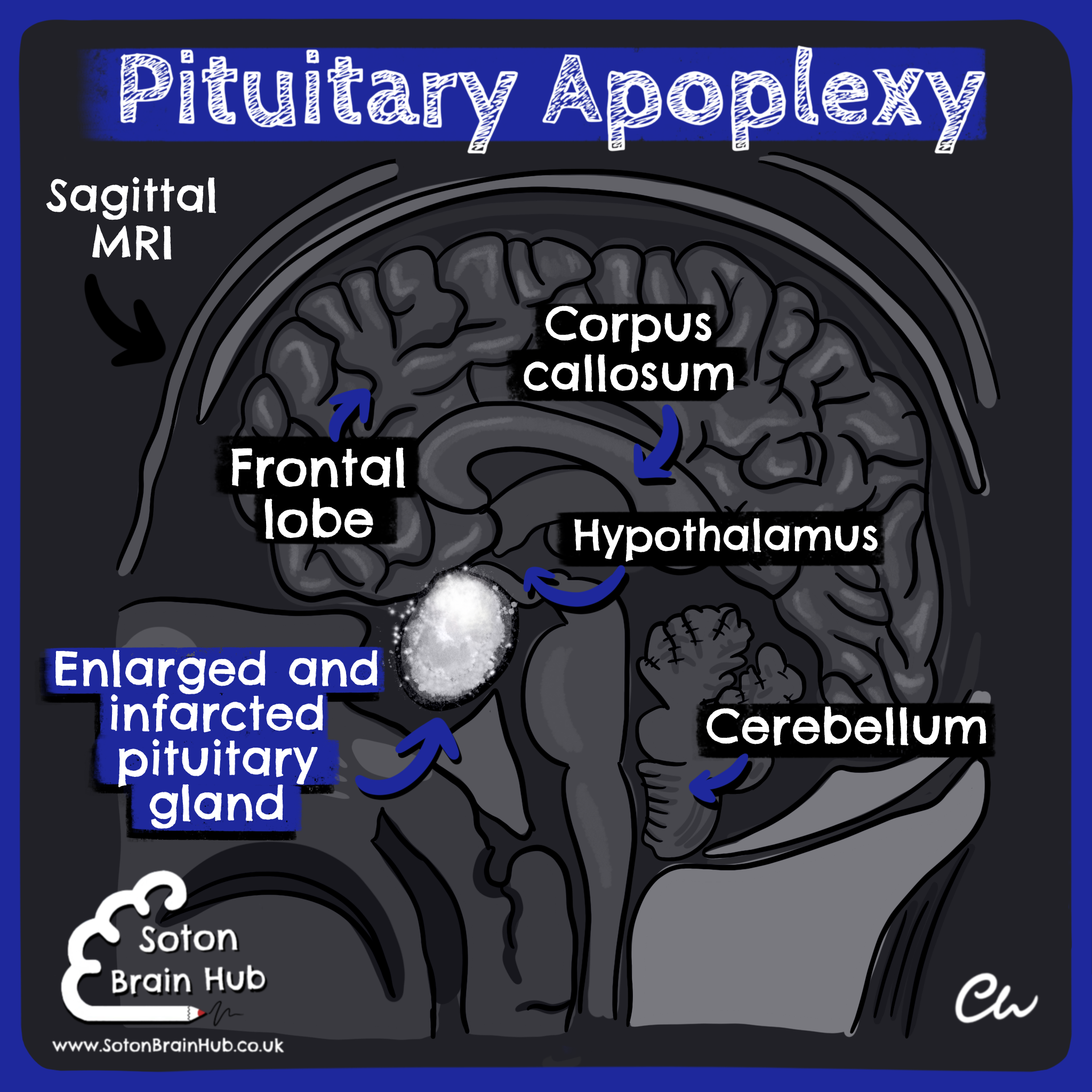 se is during hypoperfusion of the pituitary gland secondary to extensive blood loss during childbirth (termed Sheehan’s syndrome)🤱. Other risk factors include anti-coagulation, hypertension, trauma, neurosurgery and cerebral angiography. It typically presents with a sudden onset headache 🤯, visual disturbance (bitemporal hemianopia)👀, ophthalmoplegia and reduced level of consciousness.
se is during hypoperfusion of the pituitary gland secondary to extensive blood loss during childbirth (termed Sheehan’s syndrome)🤱. Other risk factors include anti-coagulation, hypertension, trauma, neurosurgery and cerebral angiography. It typically presents with a sudden onset headache 🤯, visual disturbance (bitemporal hemianopia)👀, ophthalmoplegia and reduced level of consciousness.
The patient may additionally have an Addisonian crisis due to reduced of ACTH secretion from a damaged pituitary gland. Radiologically it is best demonstrated using MRI which may show a pituitary mass with haemorrhagic (appears white due to the blood) or non-haemorrhagic (dark) infarction.
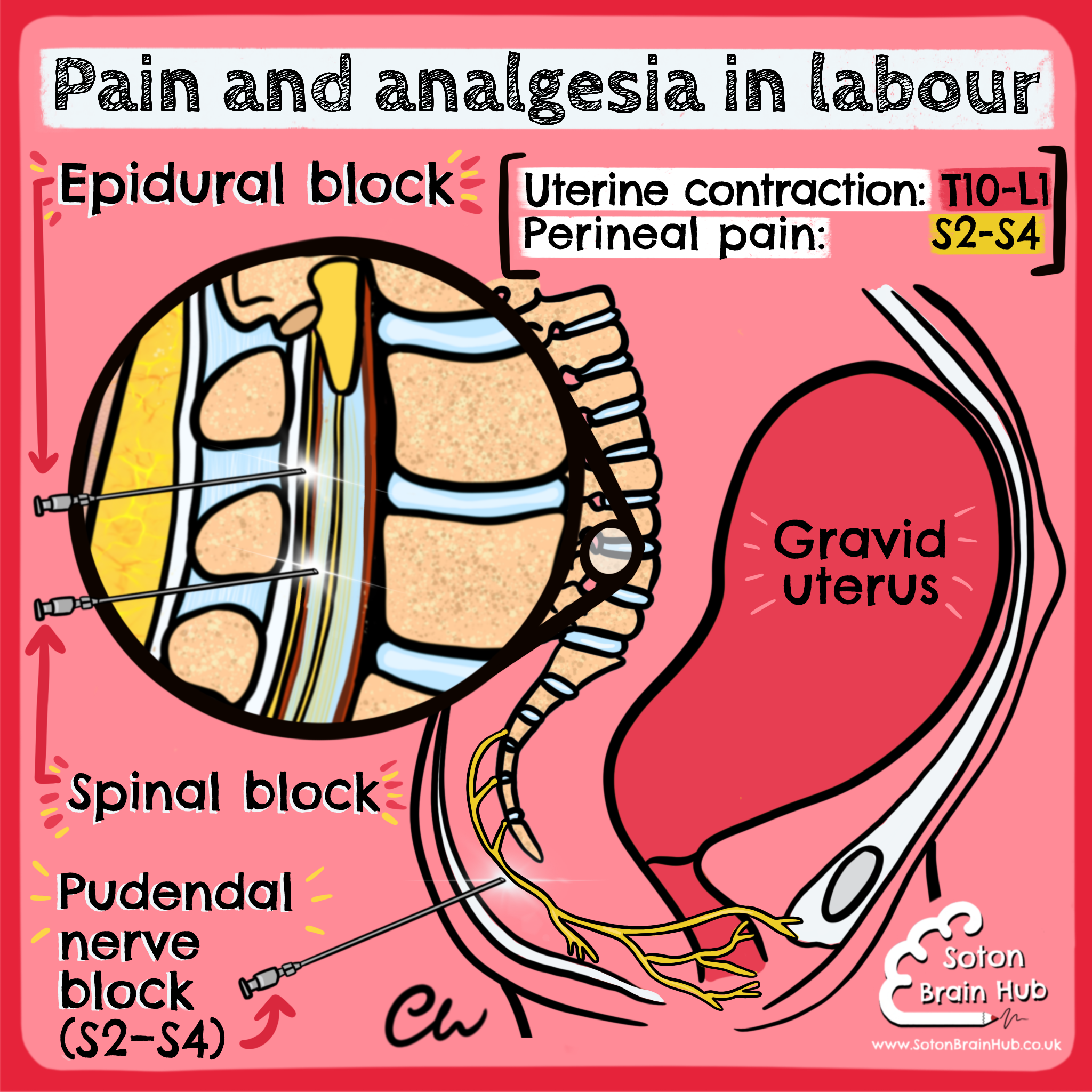
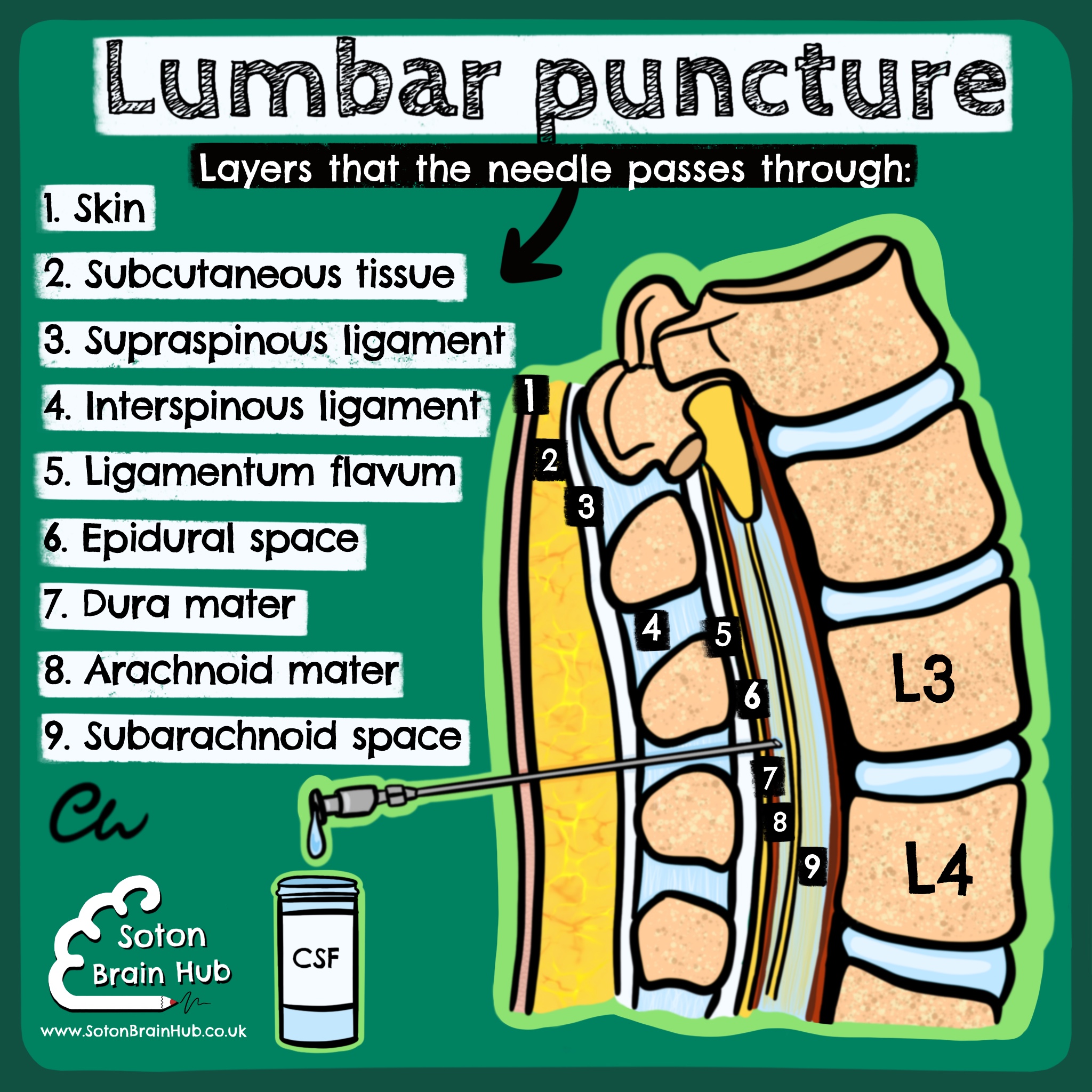
The main difference between an epidural 💉 and a spinal 💉 is the anatomy. The epidural site is outside of the CSF, while the spinal site is directly into it, making it quicker to take effect. 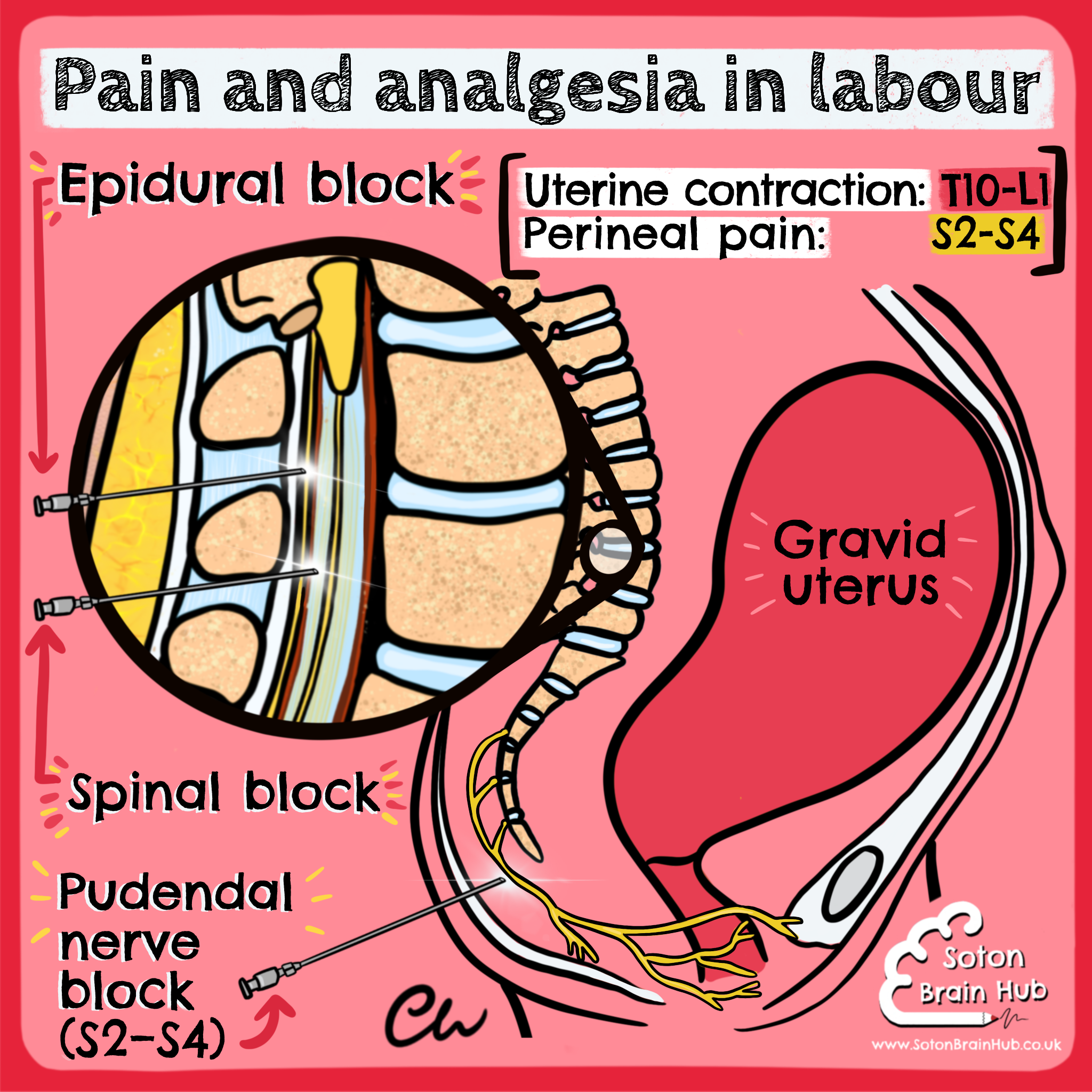
For pain relief during labour it is desirable to block the pain of contractions without effecting leg movement or the associated pushing of the baby out.🤰🏻
Spinals are usually the first choice for cesarean delivery and have more widespread effects below the injection site (most patients feel nothing).
Epidurals can be topped up which is why they are a better choice during labour, plus they still permit some sensation. Pudendal nerve blocks are for vaginal deliveries. They provide local pain relief to the perineum, but will not block it entirely.🤱🏻
Often, combinations can be used but a spinal block is a single dose only - no coming back for more 😞
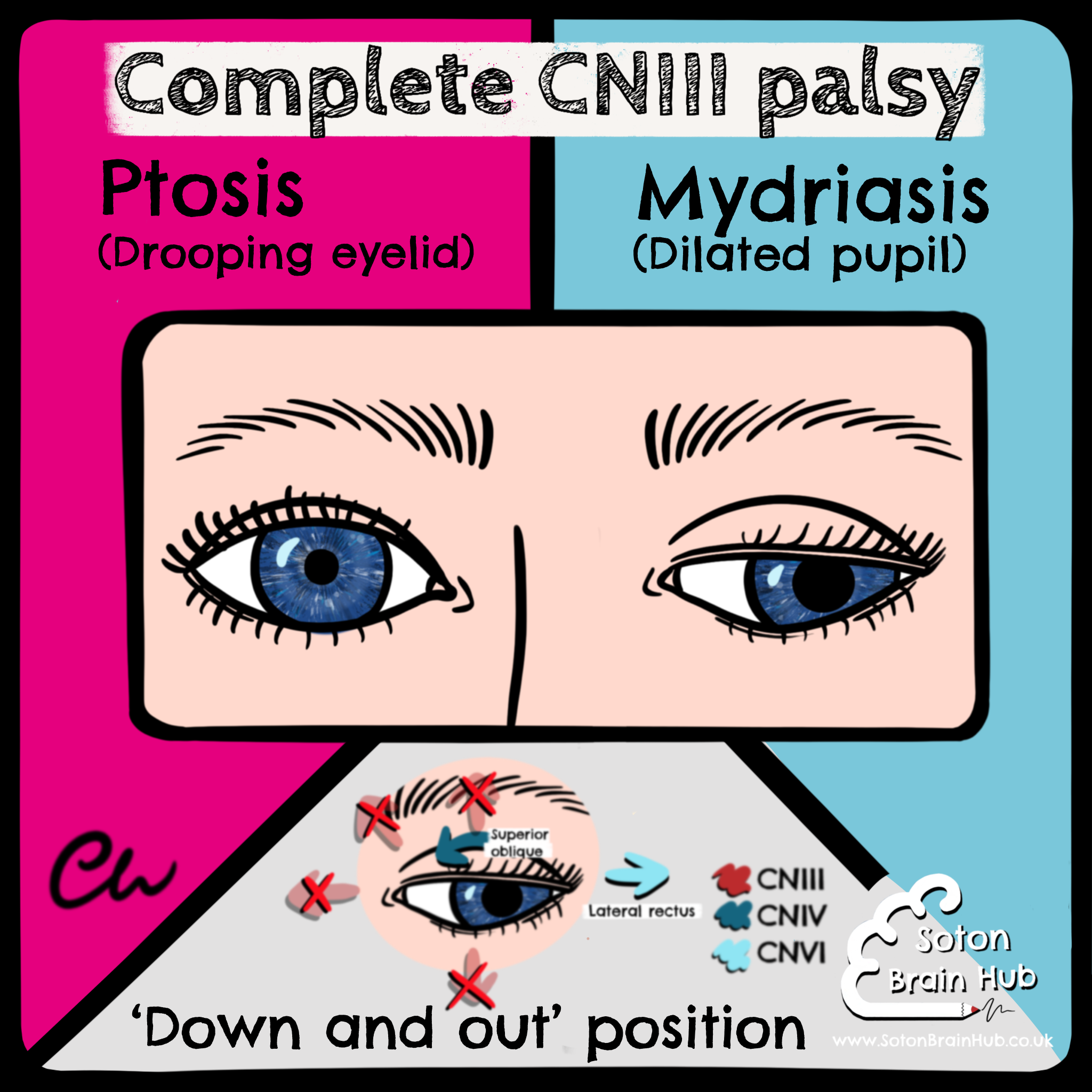
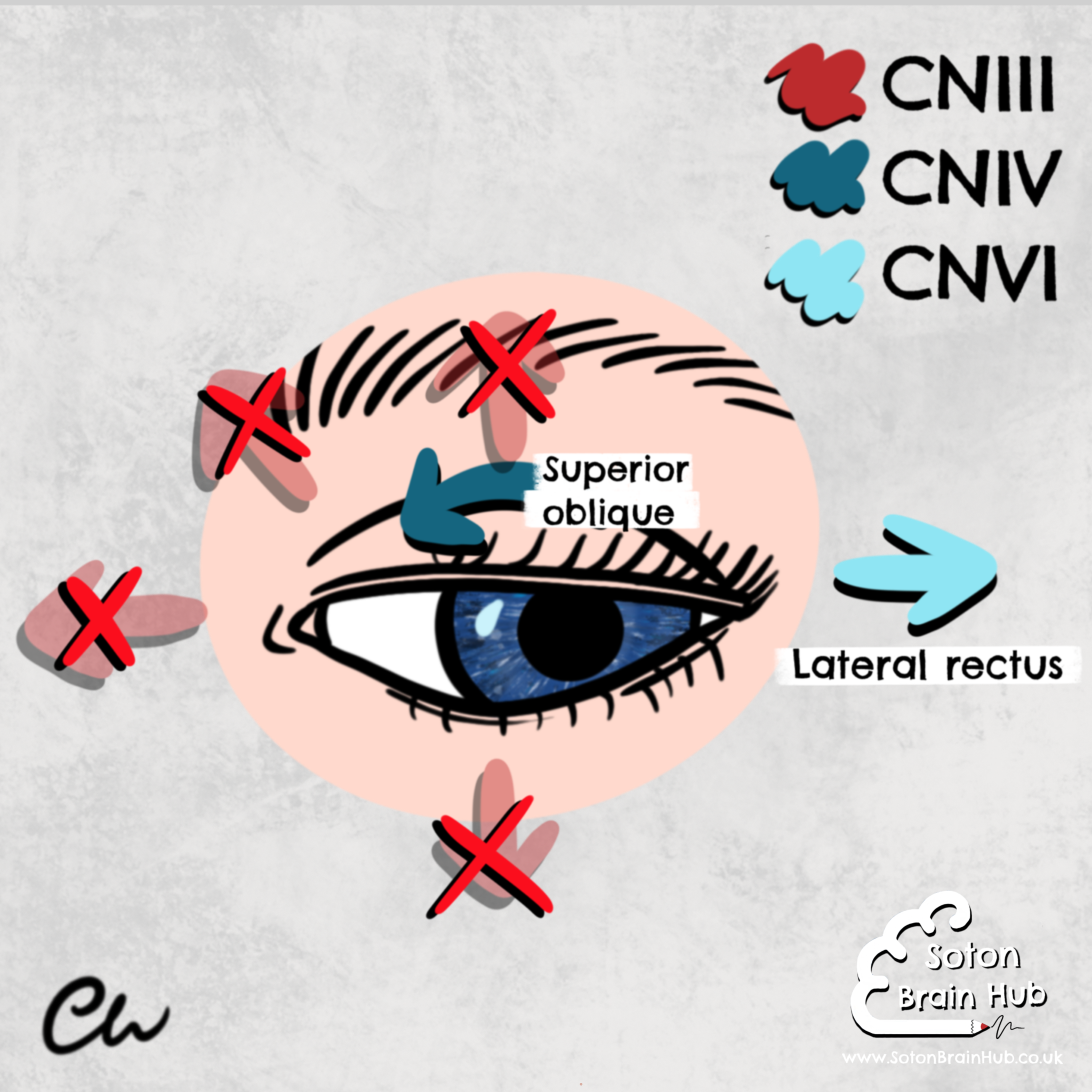
CNIII palsy causes drooping of the upper eyelid to occur because the nerve innervates the muscle controlling the upper eyelid. The affected eye will most likely deviate down and out.
This is due to the unopposed actions of the muscles not innervated by CNIII that are still working (lateral rectus and superior oblique).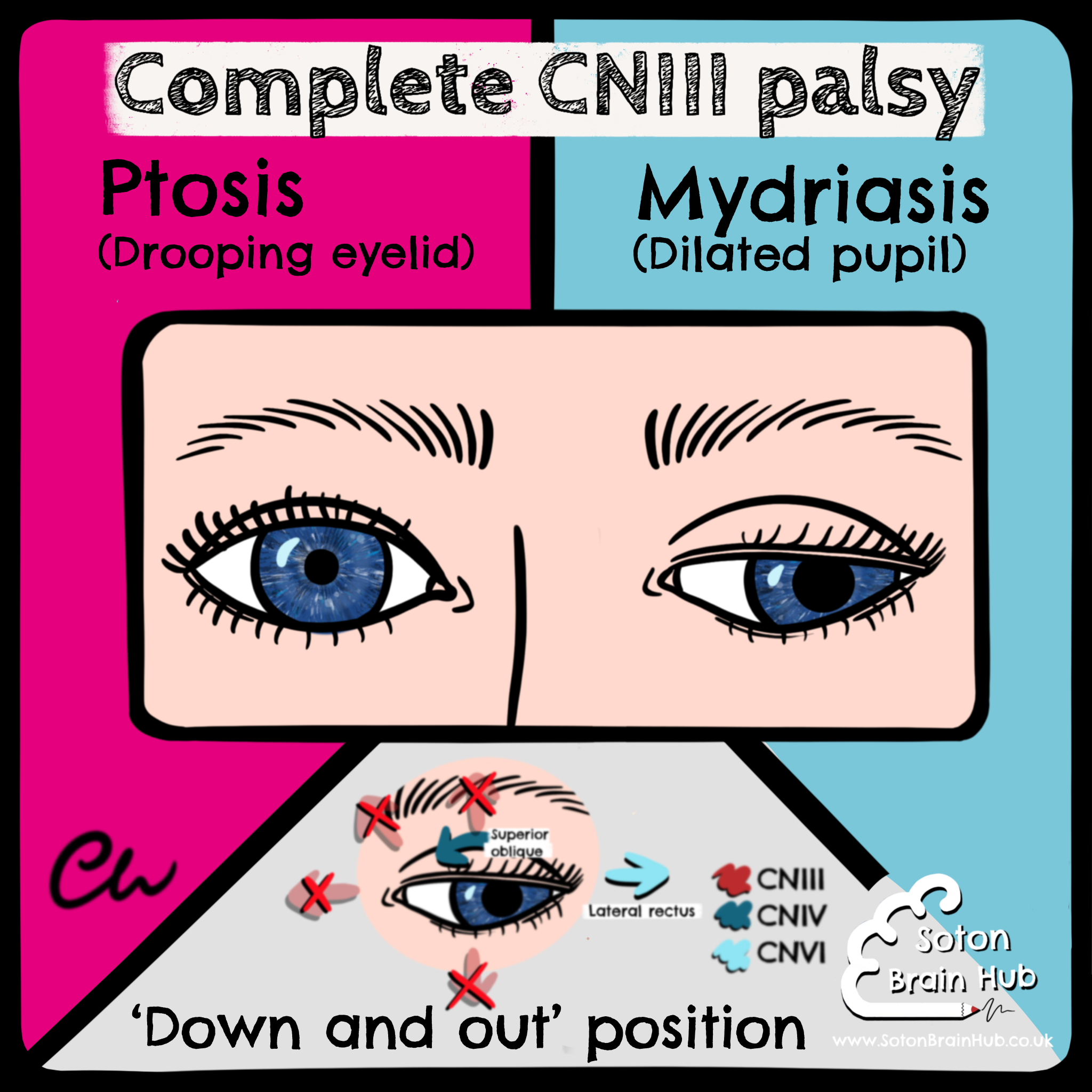
Therefore, gaze and adduction actions are slow and may not proceed past the midline. Upward gaze is also impaired 👁👁.
When downward gaze is attempted, the superior oblique muscle causes the eye to adduct slightly and rotate.
The pupil may be dilated due to unopposed action of sympathetic tone; its response to both the direct and the consensual pupillary light reflex may be sluggish or totally absent (efferent defect). 🔦